You wake up after surgery with two competing thoughts. One is relief that the arthritic pain source is finally addressed. The other is uncertainty, because now the serious work starts.
For an active adult, knee replacement recovery isn't just about getting around the house again. It's the first block of training for everything you want to return to, whether that's walking the South Shore without guarding every step, playing golf, getting back on a bike, or moving with enough confidence to rejoin the parts of life that used to feel athletic.
Table of Contents
- Your Knee Replacement Recovery is an Athletic Endeavor
- Phase 1 Immediate Post-Op (Days 1-14) Protecting the Joint and Restoring Motion
- Phase 2 Early Strengthening (Weeks 2-6) Building Your Foundation
- Phase 3 Functional Movement (Weeks 6-12) Relearning How to Move
- Phase 4 Advanced Strengthening and Return to Activity (Month 3+)
- Common Questions About Your Knee Replacement Recovery
Your Knee Replacement Recovery is an Athletic Endeavor
A lot of people approach a knee replacement like a waiting game. The surgery happens, time passes, and hopefully the knee gets better.
That mindset usually slows people down.
A better frame is this: your recovery is an athletic endeavor. You now have a structured progression, a load-management problem to solve, and a return-to-activity goal that needs to be built step by step. Those are the same principles sports physical therapists use after ACL surgery, with runners rebuilding mileage, and with dancers restoring control after time away.
For active adults, that shift matters. If your goal is only “don't hurt,” you'll often under-train. If your goal is “move well enough to trust the leg again,” your exercise choices get sharper. Range of motion matters. Strength matters. Endurance matters. Confidence under load matters too.
That's why knee replacement recovery exercises should be treated like training, not busywork. Each drill should answer a simple question: what athletic quality are we rebuilding right now? Early on, it's swelling control and muscle activation. Then it becomes force production, balance, stair control, and eventually sport-specific movement.
Practical rule: Don't judge progress only by pain. Judge it by what the knee lets you do with good mechanics.
Some active adults like using a digital coaching platform to organize home work, track consistency, and keep rehab from becoming random. That can help, especially once motivation fades and routine needs to take over.
The same logic applies in performance settings. A thoughtful strength and conditioning program for athletes works because it progresses stress instead of guessing. Post-op rehab should work the same way.
What works and what doesn't
Here's the plain version.
| Approach | Usually works | Usually backfires |
|---|---|---|
| Mindset | Treating recovery like a plan | Waiting to “feel ready” before doing enough |
| Exercise dose | Frequent, repeatable work | One hard session followed by a flare |
| Progression | Building from motion to strength to function | Skipping straight to harder activity |
| Goal setting | Tying rehab to real activities | Focusing only on the calendar |
If you want to return to sport, or even just return to movement that feels strong and normal, your knee replacement recovery exercises need to build more than basic mobility. They need to rebuild trust in the leg.
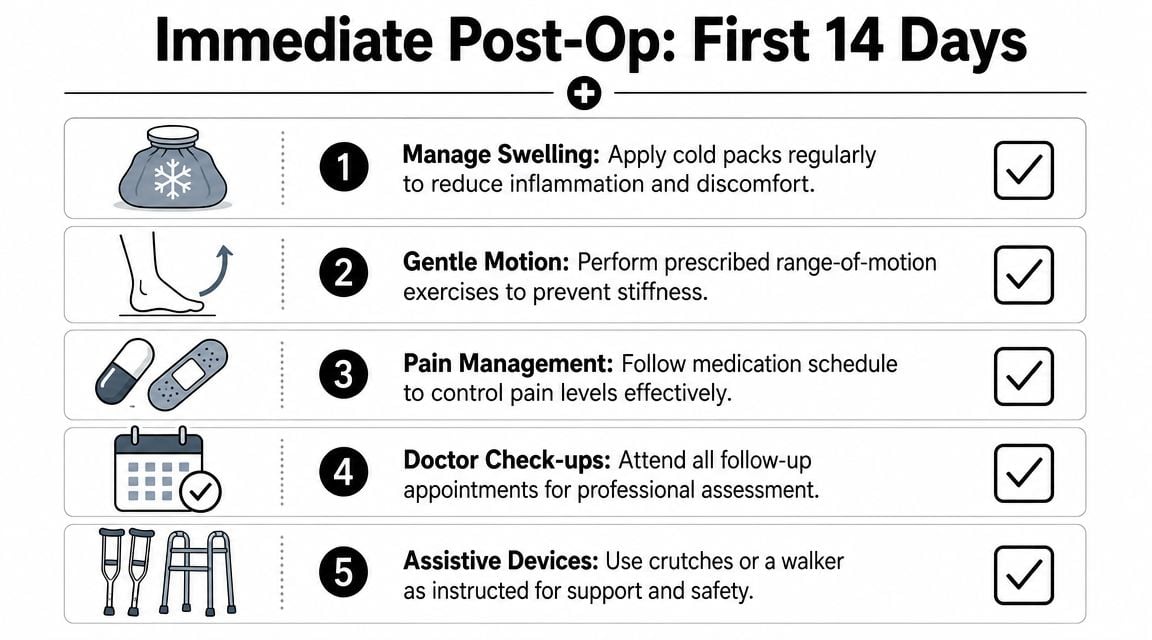
Phase 1 Immediate Post-Op (Days 1-14) Protecting the Joint and Restoring Motion
You get home from surgery motivated to make progress, then the knee feels hot, swollen, stiff, and hard to trust. That does not mean rehab is off track. It means Phase 1 has started.
For an active adult, these first 14 days are the opening block of return-to-sport training. The job is not to test toughness. The job is to build the base your later strength, balance, and sport work will depend on. That means reducing swelling, getting the knee to straighten and bend again, reestablishing quadriceps control, and walking with clean mechanics.
Win the motion battle early
In this phase, more effort is not always better. A hard session that leaves the knee more swollen can cost you motion later that day and the next morning. In practice, the best early programs use short, repeatable bouts of exercise that the knee can tolerate.
Swelling control supports performance here. If the joint stays puffy, the quad has a harder time firing and walking gets sloppy fast.
Use the standard recovery tools with a clear purpose:
- Rest between sessions so the knee settles instead of staying irritated all day.
- Ice after exercise or walking when the joint feels warm or more swollen.
- Compression if your surgeon or physical therapist wants you in a sleeve or wrap.
- Elevation to help fluid clear instead of pooling in the lower leg.
Those choices are not separate from rehab. They help you complete the next session with better motion and better muscle recruitment.
Use your walker or crutches as prescribed. A visible limp usually means the leg is not ready to accept load well yet. Good support now is better than practicing bad mechanics for a week.
If you have dealt with twisting injuries before, some of the same protection rules show up in a meniscus tear rehab program without surgery. After a knee replacement, the standard is stricter because the joint is healing from surgery and the early loss of motion can become harder to reverse if you let it linger.
Your early exercise menu
These are the exercises I want active patients to own in the first two weeks, because each one solves a specific problem that matters later.
- Ankle pumps. Move the foot up and down often through the day to help circulation and reduce stiffness from being still.
- Quadriceps sets. Tighten the front of the thigh with the knee as straight as you can comfortably manage. The goal is not just muscle tension. The goal is to reconnect the quad to knee control, which matters for walking, stairs, and eventually deceleration.
- Heel slides. Slide the heel toward you, then return to straight. This restores knee bend without forcing the joint into a flare.
- Assisted knee bends. Use a strap, towel, or the other leg if your rehab team has shown you how. This gives you a little extra flexion without turning the movement into a fight.
- Short walks. Walk around the house with the right device and an even step pattern. Several clean, short walks are more useful than one longer walk done with a limp.
One technical point matters a lot here. Work on both directions of motion. Patients often focus on bending and forget extension, but getting the knee fully straight is a major part of normal gait. If extension lags, walking stays inefficient and the knee can continue to feel blocked.
Common mistakes that slow early progress
The biggest early setbacks usually come from poor dosing or poor positioning, not from doing too little one single day.
- Do not leave a pillow under the knee for long periods. That can encourage the knee to rest in a bent position.
- Do not twist over a planted foot. Turn your whole body instead.
- Do not force sharp pain to chase bend. That often leads to guarding and more swelling later.
- Do not treat fatigue as the goal. In Phase 1, consistency beats intensity.
I tell patients to judge each session like an athlete judges training tolerance. The knee should settle after the work. If swelling keeps climbing, pain stops easing after exercise, or motion is worse the next day, the load was too high or the plan needs to be adjusted.
If that pattern shows up, contact your surgeon or licensed physical therapist rather than guessing.
Phase 2 Early Strengthening (Weeks 2-6) Building Your Foundation
By this point, it becomes evident that the problem isn't only stiffness. It's that the leg doesn't feel dependable yet.
That's especially true with the quadriceps. After knee surgery, the quad often behaves like a muscle that has forgotten its job. You try to tighten it, but the signal is weak, delayed, or inconsistent. If that doesn't improve, walking stays inefficient and stairs feel much harder than they should.
For early home rehab, a common high-yield program combines heel slides, quadriceps sets, ankle pumps, and straight-leg raises. Typical dosing from this orthopedic exercise guide is heel slides for 10 to 15 repetitions, 2 to 3 times per day, quadriceps sets held 5 to 10 seconds for 10 to 20 repetitions, 2 to 3 times daily, and straight-leg raises for about 10 repetitions, progressing toward 20 as tolerated.

Why the quad feels asleep
Swelling changes how the muscle fires. Pain changes how you load the leg. Then a compensation pattern sets in, where the other leg and the hips start doing too much.
That's why the foundation phase still leans on simple drills. Simple doesn't mean easy. It means targeted.
A practical sequence often looks like this:
- Quad sets first to improve muscle recruitment.
- Heel slides next to keep motion moving in the right direction.
- Straight-leg raises only if you can hold the knee position without a lag.
- Supported standing work after that, when the leg can handle body weight with better control.
You may also see short-arc quads added, where the knee straightens from a partially bent position over a towel or bolster. That exercise helps bridge the gap between static muscle activation and more dynamic knee control.
If the quad still won't wake up well, the answer usually isn't “try harder.” The answer is reducing swelling, improving setup, and choosing a drill the muscle can actually own.
In some cases, clinicians may use hands-on treatment or dry needling to help reduce guarding and improve how the surrounding muscles participate. That's not a replacement for exercise. It's an adjunct when the leg is struggling to re-engage.
How to progress without stirring up the knee
Progress in this window should be symptom-guided. That means you earn the next step by tolerating the current one well.
Use this quick screen:
| Green light | Yellow light |
|---|---|
| You finish the session and the knee settles | The knee feels more swollen for hours |
| Motion is the same or better the next day | Motion is clearly worse the next day |
| Walking looks smoother | You start limping more after exercise |
When that green-light pattern is consistent, standing exercises become more useful. Supported mini-squats to a shallow depth, controlled weight shifts, and basic sit-to-stand work start connecting strength to real function.
What doesn't work here is jumping ahead because the incision looks better or because you're tired of the basics. Your knee doesn't care whether an exercise is exciting. It cares whether the load matches the tissue tolerance.
Phase 3 Functional Movement (Weeks 6-12) Relearning How to Move
Here, the work starts looking less like post-op rehab and more like movement training.
The biggest shift is that strength has to transfer into tasks you care about. Getting out of a chair. Climbing stairs without pulling on the railing. Walking longer distances with an even stride. For active adults in Plymouth, Taunton, and nearby South Shore Massachusetts communities, this is often the stage where the knee starts to feel useful again, but not yet automatic.

Guidance from Hospital for Special Surgery describes progressing functional exercises in a load-managed way with sit-to-stand, supported mini-squats, and step-ups, while avoiding knee collapse and excessive depth too early in the process, as outlined in its post-knee-replacement exercise guidance.
Strength has to show up in daily movement
A strong leg on the table can still move poorly on the floor. That's why this phase emphasizes closed-chain work, where your foot is planted and the whole limb has to coordinate.
A practical movement menu includes:
- Sit-to-stand from a chair. Start with a higher surface if needed. The goal is equal contribution from both legs, not launching up with the non-operative side.
- Supported mini-squats at a counter. Keep the bend shallow at first and let the hips move back.
- Step-ups on a low step. Drive through the surgical leg, then control the lowering phase.
- Wall squats to a comfortable depth if they're tolerated well.
- Walking progression with attention to stride symmetry and push-off.
People who eventually want to jog, hike, or return to court sports often benefit from learning how running mechanics and loading patterns work long before they attempt impact again. That's why broader resources on physical therapy exercises for runners can be useful later in the return-to-activity process, even if you're not running yet.
Movement quality matters more than doing more
Most compensations in this phase are easy to spot once you know what to watch for:
- The knee caves inward
- The trunk shifts away from the surgical side
- The non-operative leg does the bulk of the work
- Depth increases before control is there
These aren't minor details. They're the difference between rebuilding capacity and rehearsing bad patterns.
The target isn't just completing the rep. The target is completing the rep with a knee position you'd trust on stairs, on uneven ground, or during a quick change of direction.
Stationary cycling is often useful here as a low-impact way to build motion tolerance and endurance. It won't replace strength work, but it can support it.
A quick demonstration can help many people clean up their step mechanics and loading strategy:
The right question in this phase is no longer, “Can I exercise?” It's, “Can I move under load without cheating?” That's the standard that carries over into sport and into everyday confidence.
Phase 4 Advanced Strengthening and Return to Activity (Month 3+)
Once basic function is in place, many people stop too early. They can walk, manage stairs, and do the essentials, so they assume they're done.
For an active adult, that's usually where lingering limitations come from.
Better outcomes often come from a more progressive approach. A randomized study published in JOSPT found that an early high-intensity rehab program produced better short- and long-term strength and functional performance than a lower-intensity program, without worsening range of motion or causing musculoskeletal injuries in the study group, as described in the study report. The same body of guidance supports resistance work commonly starting at 4 to 6 weeks and continued home exercise 2 or 3 times per week for 8 to 10 months to maintain gains.
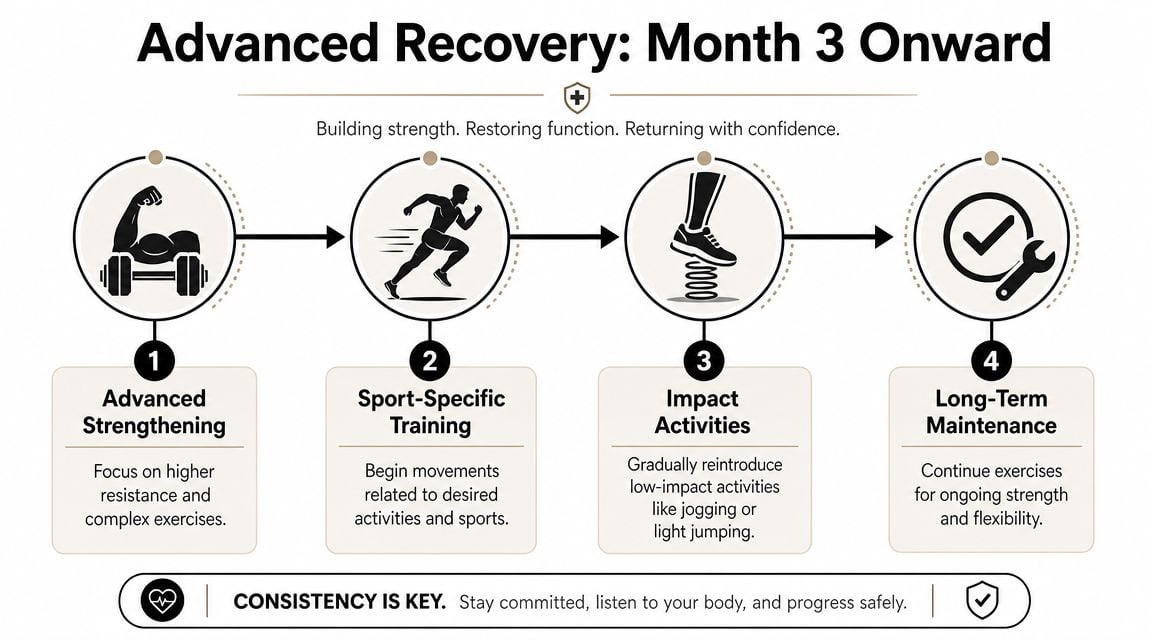
This is where rehab becomes training again
At this stage, the conversation shifts from “Can your knee tolerate activity?” to “What does your activity require?”
That's different for everyone:
- The golfer needs rotational control, walking tolerance, and enough leg strength to stay stable through a long round.
- The recreational tennis player needs deceleration, direction changes, and confidence on split steps.
- The cyclist needs repeatable force production and tolerance for sustained knee flexion.
- The dancer needs control, alignment, and graded exposure to deeper positions.
Those goals can't be met with only basic bed exercises and casual walking. They require advanced strengthening, usually with bands, machines, free weights, and more demanding balance work.
How active adults bridge back to sport
A useful late-stage program often includes a mix of:
- Leg press or squat variations with a controlled range and load that matches your form
- Hamstring curls and calf work to support the chain around the knee
- Single-leg balance drills because confidence on one leg matters in almost every sport
- Lateral movement patterns once straight-line control is solid
- Sport-specific drills that mimic the positions and pacing of your real activity
Not every person with a knee replacement will return to every sport the same way. That decision should be individualized with your surgeon and a licensed physical therapist. But the principle is the same either way. If you want to do more than basic daily life, your knee replacement recovery exercises have to prepare you for more than basic daily life.
This is also where objective testing becomes valuable. Running gait analysis can identify movement habits that overload the knee. Dance therapy can help active performers rebuild control in sport-specific positions. Return-to-sport testing gives clearer criteria for whether strength, balance, and movement quality match the activity you're trying to resume.
Don't confuse being cleared for activity with being prepared for it. Clearance is a medical threshold. Preparedness is a performance threshold.
For many active adults, month three isn't the finish line. It's the point where the plan finally starts to look like the life they want back.
Common Questions About Your Knee Replacement Recovery
The day-to-day questions during rehab are often the ones that create the most anxiety. Here are the answers patients ask for most often.
FAQ
Q. How do I tell the difference between productive discomfort and a bad response?
A little soreness during or after exercise can be normal. A bad response is when pain keeps building, swelling clearly increases, walking gets worse, or your motion is more limited the next day. Productive rehab usually leaves the knee feeling worked, not angry.
Q. How much swelling is normal?
Some swelling is expected after surgery and often increases when activity jumps too quickly. The key is the pattern. If swelling settles with rest, ice, compression, elevation, and a reasonable exercise dose, that's different from swelling that keeps escalating or comes with unusual heat, drainage, or a sharp decline in function.
Q. When can I kneel on my new knee?
This varies a lot. Some people regain tolerance to kneeling with time and graded exposure, while others find it uncomfortable even when the knee is functioning well. The bigger issue is whether the tissues tolerate the pressure and whether your surgeon has any specific restrictions. Don't force kneeling early just to prove you can.
Q. Is walking enough for rehab?
No. Walking is useful, but it doesn't fully replace motion work, quad strengthening, balance training, and functional loading. People who rely on walking alone often regain basic endurance before they regain enough strength and control for higher-level activity.
Q. When is it safe to drive again?
That depends on which knee had surgery, what vehicle you drive, whether you're still taking medications that affect reaction time, and whether you can move your leg quickly and safely. Your surgeon should clear this individually.
Q. What if my quad still feels weak months later?
That's common, especially if swelling stayed high for a while or strengthening never progressed enough. It usually means the plan needs to become more targeted and more progressive, not abandoned.
Q. Should I push range of motion hard every day?
No. Work on motion consistently, but don't attack it. Forcing bend or straightening into significant pain often creates more guarding and swelling, which can slow progress.
Q. When should I call my surgeon or physical therapist?
Reach out if pain spikes sharply, swelling escalates and doesn't settle, the incision changes in a concerning way, you lose motion compared with prior days, or walking suddenly worsens. Any symptom that feels out of proportion deserves a real conversation, not guesswork.
Knee replacement recovery exercises work best when they're individualized. General timelines help, but your body's response matters more than what someone else did. If you're unsure whether you're progressing appropriately, get assessed by a licensed PT who can look at strength, movement quality, swelling, and your actual return-to-activity goals.
If you're looking for athlete-centered guidance after knee replacement in Bridgewater, Massachusetts, Buzzards Bay, or Middleborough, Physical Therapy U can help you build a plan that goes beyond basic recovery. Our licensed DPTs work with active adults, runners, dancers, and post-surgical patients using sport-specific rehab, dry needling, running gait analysis, dance therapy, and return-to-sport testing to help you move with confidence again.
{kind=link}