You're training hard, but something still feels off. Your squat looks fine in the mirror, yet your knees cave when the weight gets heavy. Your shoulder strength is solid, but your throwing arm tightens up after practice. Your mileage is up, but the same calf or hip keeps barking.
That's usually not a conditioning problem first. It's often a movement quality problem.
In sports physical therapy, a functional movement assessment helps identify the weak link that's stealing force, efficiency, or control. For athletes, runners, dancers, and post-op patients, that matters because performance isn't just about how much strength you have. It's about whether you can express that strength cleanly, repeatedly, and under load.
At an athlete-centered clinic in South Shore Massachusetts, this is the difference between handing someone a generic exercise sheet and building a plan that fits the sport, the body, and the goal.
Table of Contents
- What Is a Functional Movement Assessment
- The Functional Movement Screen Explained
- Beyond the Screen What Your PT Actually Sees
- Interpreting Results to Build Your Performance Plan
- Who Benefits from a Movement Assessment
- Your Assessment at Physical Therapy U
- Frequently Asked Questions
- Do I need a doctor's referral to start physical therapy in Massachusetts
- Is a functional movement assessment covered by insurance
- How is this different from what a personal trainer does
- Should I get assessed even if I'm not in pain
- How often should movement be reassessed
- What should I wear to an evaluation
What Is a Functional Movement Assessment
A functional movement assessment is a structured look at how your body handles basic patterns like squatting, stepping, reaching, rotating, pushing, and balancing. For an athlete, that's not academic. Those patterns sit underneath sprinting, cutting, landing, lifting, throwing, dancing, and changing direction.
Why movement quality matters
Think of your body like a performance car. You can have a strong engine, great tires, and plenty of fuel, but if the alignment is off and one wheel is compensating for another, you won't get clean speed. You'll burn energy, lose control, and eventually something will wear down.
That's how movement works in sport. A functional movement assessment looks for the places where you're leaking force or borrowing motion from the wrong area.
A good assessment isn't a pass or fail event. It's a way to answer practical questions:
- Where are you restricted: Are your ankles, hips, thoracic spine, or shoulders limiting your mechanics?
- Where are you unstable: Can you control the range you already have, or do you collapse under speed and load?
- Where are you compensating: Are you twisting, shifting, arching, or guarding to get through the task?
- What matters most for your sport: A baseball player, distance runner, dancer, and ACL athlete don't need the same plan.
Practical rule: If your training keeps hitting the same wall, don't just add more effort. Check the movement pattern that effort is flowing through.
What a good assessment is actually looking for
In sports PT, movement quality comes before chasing volume. If you can't own a pattern unloaded, it usually shows up more clearly when the sport gets faster.
That's why clinicians look at more than flexibility or strength in isolation. They look at timing, symmetry, joint sequencing, balance, breathing strategy, trunk position, and how one region affects the next.
A useful functional movement assessment helps answer things like:
| Athletic problem | What the assessment may reveal |
|---|---|
| Recurrent knee irritation with squats or jumps | Limited ankle motion, hip control loss, trunk shift |
| Shoulder tightness with overhead sport | Thoracic stiffness, scapular control deficit, protective guarding |
| Repeated hamstring or calf overload | Poor pelvic control, stride mechanics issues, limited hip motion |
| Plateau in lifting or sprint mechanics | Force leaks through asymmetry or poor coordination |
For athletes in Bridgewater, Massachusetts, and across nearby communities like Plymouth, Taunton, East Bridgewater, West Bridgewater, Raynham, Buzzards Bay, and Middleborough, this kind of assessment is often the missing step between “working hard” and moving better.
The Functional Movement Screen Explained
An athlete can look strong in the weight room and still lose force through basic patterns. The Functional Movement Screen, or FMS, helps expose that gap.
The FMS is a standardized screen built around seven movement patterns. It gives the clinician a shared starting point for spotting mobility restrictions, stability limits, asymmetries, and control problems that can interfere with training. At PTU, that matters because a screen is not the endpoint. It is one piece of a broader functional movement assessment that helps us decide what deserves a closer look.
What the screen includes
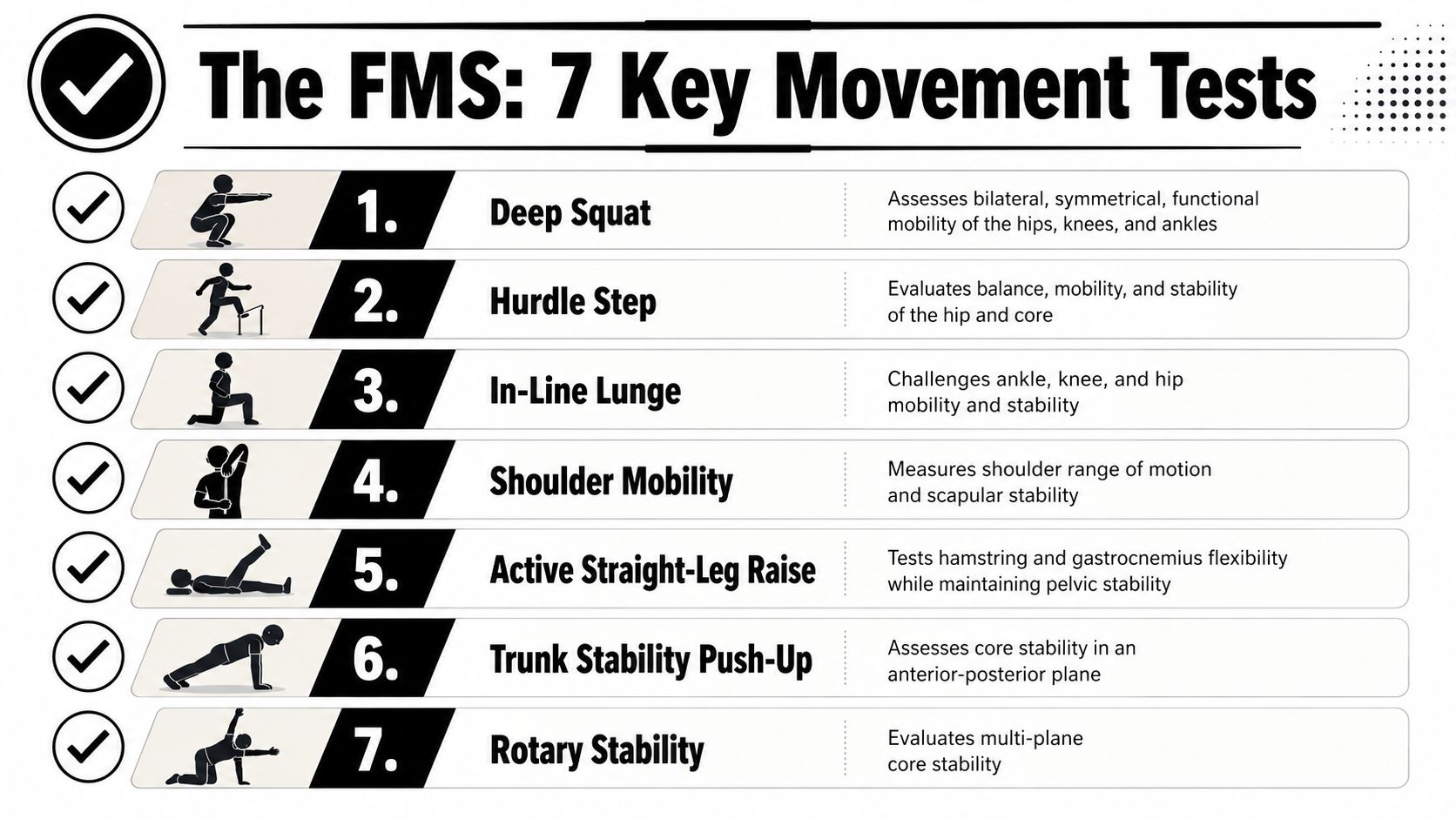
Each test places the athlete in a position that asks for joint motion, trunk control, balance, and coordination under simple constraints. The seven tests are:
- Deep squat: Looks at how the ankles, knees, hips, trunk, and shoulders work together in a full-body pattern.
- Hurdle step: Challenges balance and single-leg control while one leg moves and the other stabilizes.
- In-line lunge: Puts the lower body and trunk in a narrow, demanding position to expose control problems.
- Shoulder mobility: Assesses upper-quarter motion and how well the shoulder complex moves as a system.
- Active straight-leg raise: Gives insight into leg motion while the trunk and pelvis stay controlled.
- Trunk stability push-up: Screens how well the athlete controls the torso during an upper-body effort.
- Rotary stability: Challenges cross-body coordination and multi-plane trunk control.
This format is useful because it is repeatable. A sports PT, strength coach, and athlete can all look at the same pattern and speak the same language about what improved, what stayed limited, and what still breaks down under load.
That is also why the FMS should stay in its lane. It is a screen. It does not replace sport-specific testing, strength testing, or a closer look at movement in context, such as a running gait analysis for athletes with stride-related breakdowns.
Later in the process, it helps to see the movements in action:
How scoring works
Each movement is scored from 0 to 3, with a total possible score of 0 to 21. Higher scores reflect cleaner movement within the test criteria. Lower scores point to compensation, limited motion, loss of balance, or inability to complete the pattern as instructed.
The number alone does not tell an athlete why the movement broke down. Two athletes can post the same score and need very different plans. One may need ankle mobility. Another may have plenty of motion but poor control when the trunk and pelvis have to organize together.
That distinction matters in sports rehab and performance. A generic screen can identify a pattern worth flagging. A Doctor of Physical Therapy uses the pattern, the compensations, the athlete's sport, and the injury history to decide what to train next.
Foot behavior is a good example. If the arch collapses, the toes lose contact, or the athlete cannot create pressure through the ground, the whole chain above it can change. That is one reason many sports clinicians pay close attention to the feet during screen-based testing, and why resources like Dr Emily Splichal on foot health are useful for understanding how foot function shapes movement quality.
At PTU, the best use of the FMS is simple. It gives us a clean starting snapshot, then we build from there with a more individualized assessment that matches the athlete in front of us.
Beyond the Screen What Your PT Actually Sees
An athlete can score the same as someone else and have a completely different problem. That's why the checklist alone doesn't carry the fundamental value. The value is in the interpretation.
The score is only the start
A sports PT watches the movement the same way a skilled coach watches a lift. Did the athlete complete the rep? Sure. But how did they get there?

A low-quality squat, for example, might come from several different drivers:
- Joint mobility loss: The ankle doesn't bend enough, so the heel lifts or the knees dive inward.
- Poor motor control: The athlete has the range, but can't organize the trunk and pelvis under demand.
- Asymmetry: One hip shifts, one foot turns out, or one side loads differently than the other.
- Protective strategy: The body avoids a motion because it doesn't trust it, even before pain shows up.
That's why foot and ankle behavior matters so much. If you want a deeper look at how the feet influence the rest of the chain, this discussion from Peak Performance featuring Dr Emily Splichal on foot health is worth your time.
Why detail matters for athletes
For runners, this gets even more specific. A clinic-based movement assessment often pairs well with a more sport-specific look at stride mechanics, ground contact, and force transfer through running gait analysis.
The body doesn't care what you meant to do. It responds to what you repeatedly load.
That's the main difference between a generic screen and a clinical assessment. A Doctor of Physical Therapy isn't just labeling a pattern as good or bad. They're separating the reason from the symptom. That distinction changes everything about what comes next.
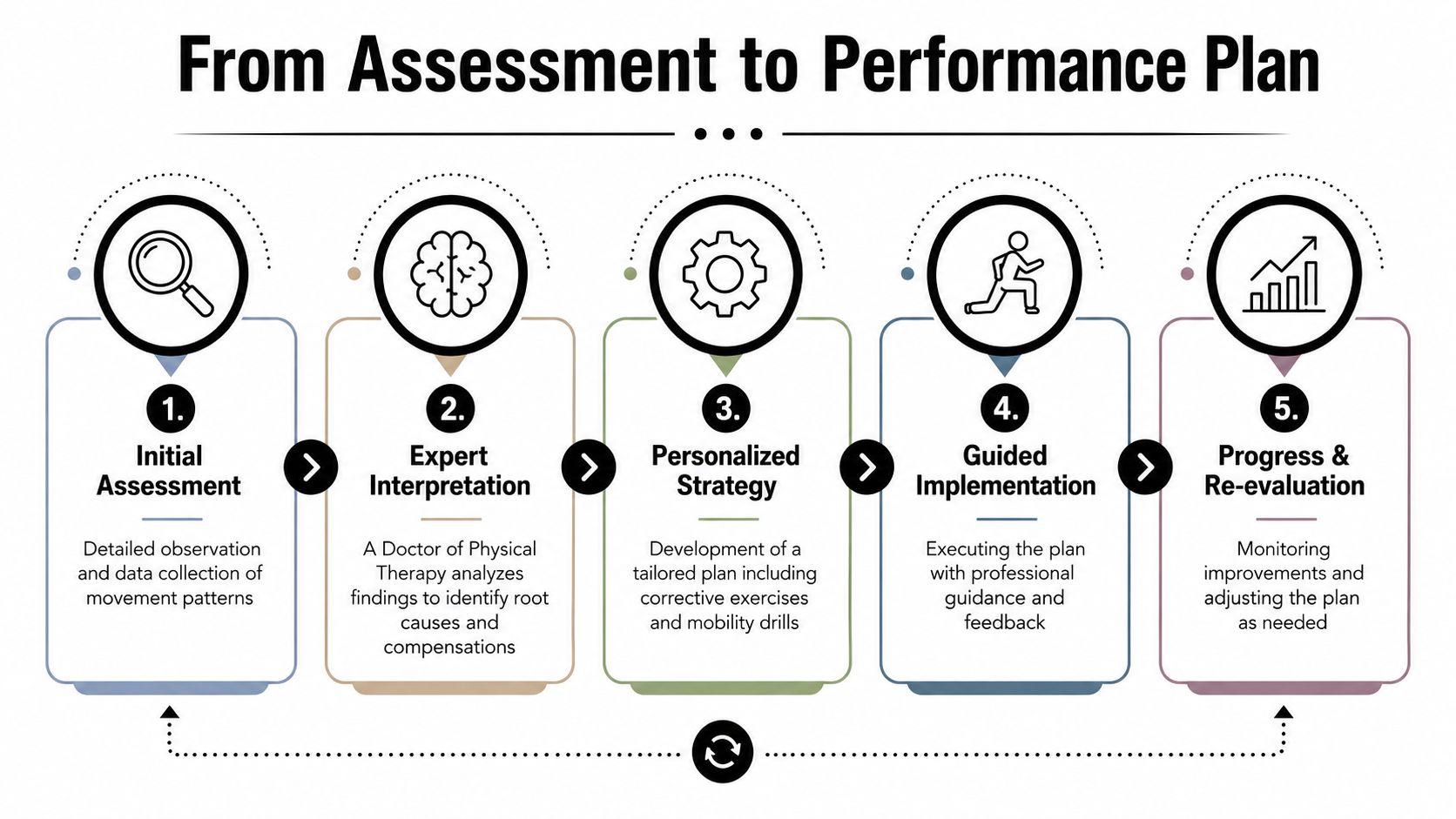
Interpreting Results to Build Your Performance Plan
You finish a lift session, and the bar speed looks fine until the load climbs. Then the knees cave, the rib cage flares, and the rep turns into a grind. That result matters because the training plan has to answer the breakdown you show, not the one someone guessed from across the gym.
Assessment findings matter when they change decisions. For an athlete, that means tying a movement issue to a sport goal, whether the target is a harder first step, cleaner change of direction, better force transfer in a deadlift, or a safer return after surgery. At PTU, that is where a screen becomes an assessment. We do not stop at scoring a pattern. We use the pattern, the sport, the injury history, and the training demand to decide what gets trained first and what can wait.
How findings change the plan
A useful plan starts with the limiter that is costing performance.
If a swimmer or baseball player loses position overhead, extra band work may miss the point. The better answer might be thoracic mobility, scapular control, manual treatment, or dry needling when the presentation supports it. After that, the athlete has to own the new range under load and then carry it into pressing, throwing, or acceleration work. Range that only shows up on the treatment table does not help on game day.
If a squat breaks down, the correction depends on the driver and the sport demand:
- Ankle motion is limiting the pattern: Restore dorsiflexion, then re-test the squat with tempo and load.
- The trunk cannot control force: Build anti-extension and anti-rotation strength, then return to squatting with a progression the athlete can keep clean.
- Hip control is the weak link: Coach femur and pelvis control before chasing more depth.
- The pattern collapses once speed enters the picture: Progress from controlled reps to landing, deceleration, and reactive drills.
Recovery habits shape the result too. An athlete who trains hard but sleeps poorly or under-recovers often looks stiff, slow, and less coordinated the next day. For athletes asking how sleep and supplementation fit into readiness, this overview of athlete recovery supplements is a useful non-clinical companion to the rehab process.
Once mobility and control improve, many athletes still need a structured bridge back to performance. A sport-specific strength and conditioning program for athletes helps turn better movement quality into usable speed, power, and durability.
When pain changes the assessment
Pain changes interpretation.
At that point, the question is not just whether the movement looks clean. The question is whether pain is distorting the pattern, protecting a tissue, or exposing a capacity problem the athlete can no longer hide. A painful toe touch, lunge, or rotation test has to be broken down with more precision, because the same ugly pattern can come from stiffness, weakness, irritability, or a true tissue issue.
That is where sports PT judgment matters most. A generic screen can flag risk. A full movement assessment helps determine whether the athlete needs load reduction, tissue-specific treatment, motor control work, or a return to strength. In the South Shore athlete population we treat at PTU, that distinction changes timelines and programming all the time. The right exercise at the wrong stage can keep an athlete stuck. The right progression, matched to the actual limiter, gets them back to training with more confidence and less wasted work.
Clinical takeaway: The right exercise for the wrong problem still fails.
Who Benefits from a Movement Assessment
Not every athlete presents the same way, but the value of a functional movement assessment shows up quickly when the demand of the sport is clear.
The youth athlete
Youth athletes often compensate well enough to keep playing, especially when they're fast or naturally strong. The issue is that they can build a lot of performance on top of a shaky base.
A middle school or high school athlete may squat shallow, land stiff, rotate poorly, or lose balance on one side without anyone catching it until pain shows up. Cleaning that up early can make sport-specific training more productive and helps build better habits before sloppy mechanics get reinforced season after season.
The adult runner
Adult runners usually care about one thing first. Can I run consistently without the same issue coming back?
Movement assessment helps when the runner who lives in Plymouth, Raynham, or Taunton keeps cycling through calf tightness, hip irritation, or recurring knee pain despite doing mileage and strength work. Sometimes the issue isn't effort. It's that the body is finding the same inefficient path every step.
The dancer
Dancers are a different category. They often have range that other athletes want, but range without control can create its own problem.
For dance therapy, the assessment has to respect turnout demands, single-leg control, spinal motion, foot mechanics, and the difference between usable mobility and hanging on passive range. A dancer may look flexible enough in class and still lack the stability needed to repeat that motion safely under fatigue.
The post-surgical athlete
Post-op athletes, especially after ACL reconstruction, need more than time-based milestones. They need to know whether the movement system is ready.
That's where functional assessment supports return-to-sport testing. If the athlete can produce force but still unloads one leg, rotates away from the surgical side, or hesitates with deceleration, the risk isn't gone just because the calendar moved forward.
For clinicians looking at sports rehab pathways more broadly, some therapists explore settings through resources on traveling therapy jobs to see how different systems approach athlete care. For the athlete in front of you, though, the takeaway is simple. The assessment has to match the sport, the demand, and the phase of recovery.
Your Assessment at Physical Therapy U
At Physical Therapy U, the assessment isn't a standalone screen done in a corner of the gym. It's part of a full one-on-one evaluation with a licensed Doctor of Physical Therapy who understands sports performance, rehab progression, and return-to-sport demands.
Athletes who come to PTU in Bridgewater, Massachusetts, Buzzards Bay, or Middleborough can expect a process that connects the movement findings to the actual goal. That might mean running analysis for a distance athlete, dance therapy for a performer, dry needling and manual treatment for an irritated tissue, or structured testing after ACL rehab.
The point isn't to hand you a score and send you home. The point is to figure out what's limiting you, what's compensating, and what needs to change first so training starts working better.
If you're deciding whether sports PT is the right fit, PTU's overview of sports medicine and rehab is a good place to start. From there, the next move is simple. Book an evaluation and get a plan built around your sport, your body, and your next phase of training.
Frequently Asked Questions
Do I need a doctor's referral to start physical therapy in Massachusetts
In many cases, you can start by contacting the clinic directly. Insurance rules and your specific situation can affect the process, so it's smart to confirm the details when you schedule.
Is a functional movement assessment covered by insurance
When it's part of a standard physical therapy evaluation, it's typically handled within that broader visit rather than as a separate performance-only service. Coverage depends on your plan, your benefits, and the reason for care.
How is this different from what a personal trainer does
A good trainer coaches exercise and performance. A Doctor of Physical Therapy evaluates movement through a clinical lens, screens for pain drivers, identifies impairment patterns, and determines whether a movement issue points to mobility loss, motor control deficit, or something that needs more specific medical follow-up.
Should I get assessed even if I'm not in pain
Yes, especially if you keep hitting the same training plateau, feel one-sided, or want to improve efficiency before a season ramps up. Athletes don't need to wait for a full-blown injury to learn something useful from movement testing.
How often should movement be reassessed
It depends on the goal. Reassessment makes sense after a block of corrective work, during a return-to-sport progression, or when symptoms or training demands change.
What should I wear to an evaluation
Wear clothes you can move in comfortably. Shorts, a T-shirt, and athletic shoes usually make it easiest for the PT to observe squat mechanics, single-leg control, running patterns, or sport-specific movement.
If you're an athlete, runner, dancer, or post-op patient in South Shore Massachusetts, Physical Therapy U can help you turn movement findings into a real performance plan. Book at our Bridgewater, Buzzards Bay, or Middleborough locations to work one-on-one with a licensed DPT and start moving with more control, power, and confidence.
{kind=link}