Your ACL is healing on schedule. Your strength is coming back. The swelling is better. But your knee still feels sore, tight, or weirdly threatening when you try to jog, cut, or descend stairs.
That disconnect frustrates athletes all the time in Bridgewater, Massachusetts and across the South Shore. You start wondering if the graft is wrong, if something got missed, or if soreness means you're moving backward.
Often, it doesn't.
As sports physical therapists, we spend a lot of time teaching athletes that pain is real, but it isn't always a direct measure of damage. That idea sits at the center of Pain Neuroscience Education, or PNE. For an ACL athlete, runner, dancer, or post-op patient, it can be the difference between staying stuck in fear and building confidence again.
Table of Contents
- What Is Pain Neuroscience Education
- Understanding How Your Brain Creates Pain
- How PNE Changes Your Recovery Journey
- Using PNE for Acute and Post-Surgical Recovery
- What Pain Education Looks Like at PTU
- Athlete Stories From Our South Shore Clinics
- Your PNE Questions Answered
What Is Pain Neuroscience Education
An athlete's classic complaint sounds like this. "My surgeon says things look good. My rehab is progressing. So why does my knee still hurt?"
Pain Neuroscience Education gives a better answer than, "Just push through it," or, "If it hurts, something must be wrong." It teaches how pain is produced by the nervous system as a protective response, rather than as a simple damage meter.
That shift matters because older pain models often treated pain like a scoreboard. More pain meant more tissue damage. Less pain meant less damage. Real recovery doesn't work that neatly, especially after surgery, repetitive training loads, or a stretch of stressful rehab.
PNE developed in the early 2000s to address limits in those older models, and one widely cited evidence summary noted that 25.3 million U.S. adults were living with daily chronic pain, which helps explain why this approach gained traction in rehabilitation practice (Pain Neuroscience Education overview from Evidence In Motion).
Why athletes get confused
Athletes are used to body feedback. If your quad burns in a lift, that usually means effort. If you roll an ankle and can't bear weight, that usually means injury.
But post-op soreness, movement fear, training stress, poor sleep, and past pain experiences can all turn up the nervous system's alert level. That's where many athletes get lost. They assume every warning signal means new harm.
Key idea: Pain is protective. Sometimes it's accurately protective. Sometimes it's overprotective.
For an ACL athlete, that can look like:
- Jogging fear: Your knee aches when you start running, even though the tissue is tolerating the load.
- Cutting hesitation: Pivot drills feel dangerous before they become dangerous.
- Post-workout soreness panic: Normal rehab soreness gets interpreted like a setback.
PNE doesn't replace exercise, strength work, return-to-sport testing, or hands-on care. It makes those things easier to do with less fear and better judgment.
What PNE is not
It isn't someone telling you the pain is "all in your head."
It isn't a motivational speech.
And it isn't a substitute for a proper exam by a licensed physical therapist, especially if you're early after surgery or dealing with swelling, instability, or a true loss of motion.
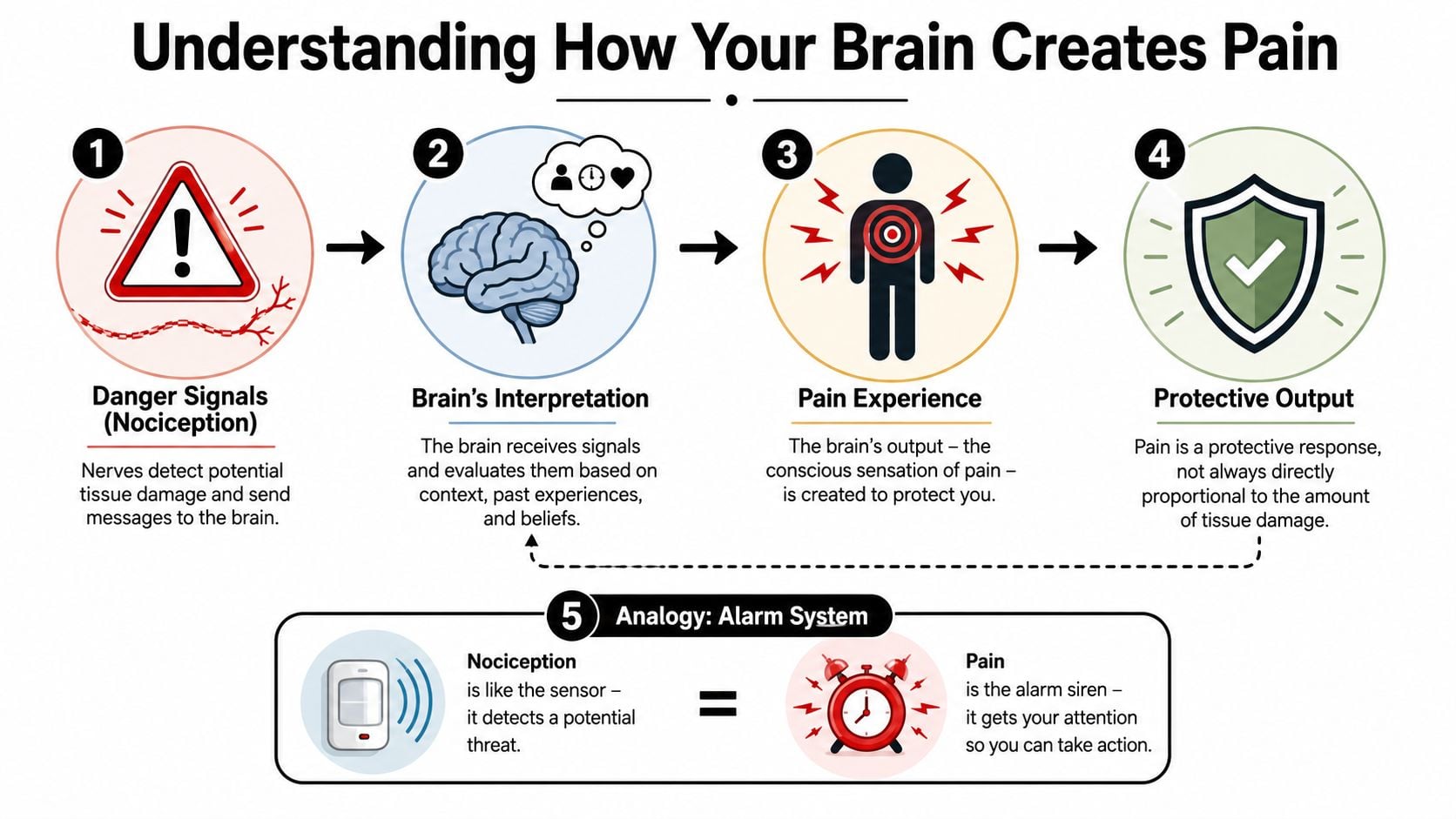
Understanding How Your Brain Creates Pain
When athletes hear that the brain creates pain, many assume that means the pain isn't real. That's the wrong takeaway.
The better takeaway is that the brain produces pain for protection. It uses information from the body, but it also weighs context, memory, stress, beliefs, and perceived threat. That helps explain why one movement can feel safe on one day and alarming on another.
Why pain and damage are not the same thing
A simple sports analogy helps. Think of nociception as the sensor in a smoke alarm. It detects possible danger. Pain is the alarm siren your system decides to sound.
Sometimes smoke means a real fire. Sometimes burnt toast sets the alarm off.
Your knee has sensors that detect mechanical and chemical changes. Those signals travel upward. Then the nervous system interprets them. If the system decides you need protecting, you feel pain, guarding, tension, or apprehension.
That means two things can be true at once:
- Your pain is completely real.
- The amount of pain you feel doesn't always match the amount of tissue damage present.
Pain is less like a photo of your knee and more like a coaching decision. The body gathers information, then the nervous system chooses how much protection to apply.
For athletes, that explains a lot of common rehab moments. A bodyweight squat can feel more threatening than a leg press because of confidence, memory, or control demands, not because the squat is automatically more damaging.
What central sensitization feels like in sports rehab
One reason PNE gets so much attention is that it tends to be most useful when pain is shaped by central sensitization or by unhelpful illness beliefs. Its purpose is to help people move away from a pure tissue-damage story and toward a nervous-system story, especially when the system has become hypersensitive. It also works best as part of a broader plan that includes exercise therapy, not as a stand-alone lecture (clinical summary on Pain Neuroscience Education from Physio-Pedia)).
Central sensitization sounds technical, but the feeling is familiar. It's like a car alarm that becomes too easy to trigger. A light touch, a small bump, or a harmless movement starts setting it off.
In rehab, that might look like:
- Lingering soreness that outlasts tissue healing
- Pain spreading beyond the original injury area
- Movement fear that rises before the movement even begins
- Flare-ups after normal training progressions
That doesn't mean every post-ACL athlete has central sensitization. It means some athletes develop a nervous system that's acting like an overprotective teammate, yelling "danger" too often.
What this means for your next workout
Once you understand pain as an alarm system, rehab decisions get clearer.
Instead of asking only, "Did I feel pain?" you start asking:
- What kind of pain was it? Sharp, unstable, hot, and escalating feels different from predictable soreness.
- What happened afterward? Did symptoms settle, or did the knee become more reactive for a prolonged stretch?
- What was the context? Poor sleep, stress, higher training load, and fear can all turn the volume up.
That mindset helps athletes train smarter. It also opens the door to graded exposure, return-to-sport drills, running gait analysis, and sport-specific progressions without treating every sensation like a threat.
How PNE Changes Your Recovery Journey
For most athletes, the first win from pain neuroscience education isn't a dramatic pain score drop. It's a behavior change.

You stop bracing for every step. You stop skipping exercises because a sore knee must mean damage. You stop interpreting normal rehab discomfort as proof that surgery failed.
A recent review found moderate-certainty evidence from 19 randomized controlled trials that adding PNE to physiotherapy improved outcomes. The pooled pain reduction was 0.784 points on a 0 to 10 scale with a 95% CI of 0.462 to 1.105, and one included intervention reported pain dropping from 5.89 to 3.03 while disability improved from 56.67 to 12.51 (review of PNE added to physiotherapy for chronic musculoskeletal pain).
What changes first
The biggest early shift is often your relationship to pain.
Instead of "pain means stop," the thought becomes, "pain is information." That doesn't make you reckless. It makes you more accurate.
Expert commentary has noted that PNE's strongest and most reproducible effects are on fear-avoidance and pain catastrophizing, while direct pain intensity change is often smaller and less consistent. The same commentary states that the minimum detectable change for pain is about 2 points on a 10-point scale, which helps explain why education can matter even when the first thing you notice isn't a huge pain-number swing (expert discussion with Adriaan Louw on Integrative Pain Science Institute).
That matters in ACL rehab because fear can be a subtle impediment to progress. An athlete who doesn't trust their knee won't load it well, won't cut decisively, and won't express normal movement. Confidence is part of function.
Why education works better with movement
Education gives the nervous system a new story. Movement proves that story is true.
That's why PNE pairs so well with sports rehab. Once you understand that a controlled step-down, sled push, landing drill, or deceleration rep isn't automatically harmful, you can train with more intent.
A few tools often fit naturally around that process:
- Graded exposure: Build from low-threat drills to higher-threat drills instead of avoiding them.
- Sleep and recovery habits: A calmer system usually tolerates load better.
- Thought reframing: If anxious thinking keeps feeding symptoms, resources like Cedar Hill's therapy guide can help you understand common approaches to changing how you respond to difficult thoughts.
- Integrated sports rehab: Education works best when it sits inside a plan that also includes strength, mobility, and progressive return-to-play work, like the principles discussed in this sports medicine and rehab article.
If you want a quick visual explanation before your next workout, this video is a useful starting point.
Using PNE for Acute and Post-Surgical Recovery
A lot of public pain education talks only about chronic pain. That's part of why post-op athletes assume PNE isn't relevant to them yet.
That assumption misses an important clinical point. Newer reviews describe acute pain PNE as an emerging area, separate from the much larger persistent-pain literature, and they highlight a practical question athletes ask all the time. Is this useful right after injury or surgery, or only later on? (focused review on acute pain pain-neuroscience education)
Why this matters early after ACL surgery
Early ACL rehab is full of sensations that are easy to misread. Swelling creates pressure. Quad activation feels awkward. Extension work can feel intense. A normal change in workload can make the knee ache later that day.
Without context, athletes often build a threat story around those sensations. They think, "If it hurts, I must be messing something up."
PNE helps separate expected post-op sensitivity from signs that need medical attention. It also gives patients language for a healthier rehab mindset: the knee may be irritated, sensitive, stiff, or deconditioned without being structurally harmed by every controlled exercise.
Practical rule: In rehab, some movements can hurt without causing harm. The key is matching the response to the stage of healing, the exercise dose, and the reaction afterward.
That idea supports earlier, calmer participation in the basics:
- Range-of-motion work
- Quad activation
- Walking retraining
- Gradual strength loading
- Later running and change-of-direction progressions
For athletes who want a more detailed look at timelines and common experiences, this guide on what to expect after ACL surgery can help frame the process.
A simple hurt versus harm filter
Athletes usually don't need a lecture in this phase. They need a filter.
Helpful questions include:
- Was the exercise planned and controlled?
- Did the knee feel stable during it?
- Did symptoms settle back down in a reasonable way afterward?
- Was the soreness proportional to the session?
Those questions reduce all-or-nothing thinking. They also help prevent a common spiral where fear causes guarding, guarding changes movement, and that altered movement creates even more soreness.
Sports physical therapy matters. A licensed DPT can check whether your symptoms fit expected healing, modify load if needed, and keep you progressing without guessing.
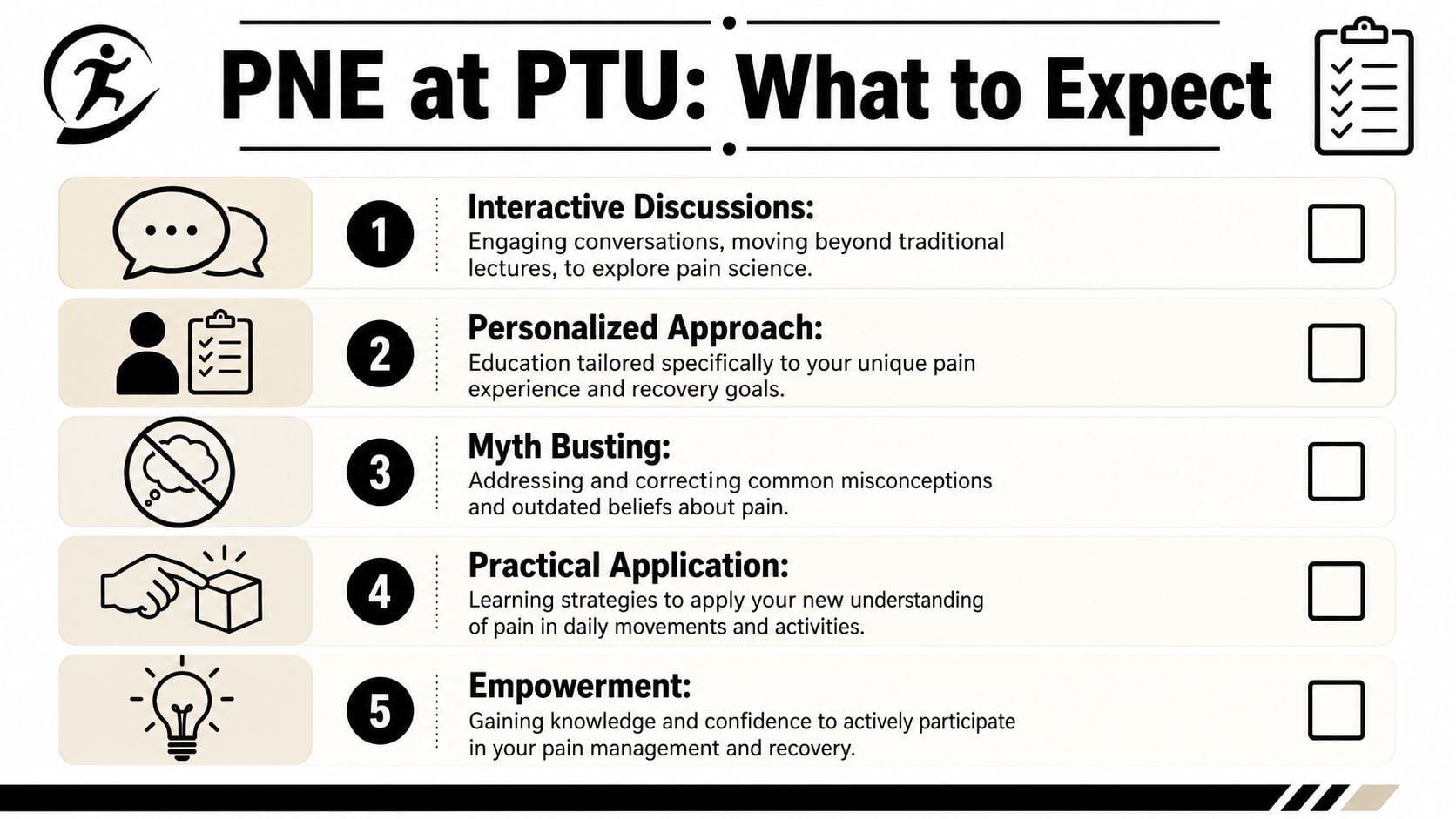
What Pain Education Looks Like at PTU
Good pain education doesn't feel like sitting through a classroom lecture. It feels like a useful conversation that changes how you move in the same session.
Research on education delivery matters here. Neutral sources note that written-only pain education is insufficient, oral education works better, and the best effects are often seen in individual sessions. Recent studies frequently use one or two sessions lasting about 30 to 45 minutes, then reinforce those ideas throughout care (IASP discussion of pain education delivery and fibromyalgia).
What happens in a real session
In a sports PT setting, the conversation usually starts with your actual complaint, not abstract theory.
A Bridgewater soccer player might say, "I can squat, but cutting scares me." A runner from Plymouth might say, "The ache always ramps up before I even start the second mile." A dancer near Taunton might say, "My hip feels pinchy, so I keep backing off."
From there, a therapist connects the science to the exact movement problem. Then you test it in real time.
That can include:
- Movement exposure: You learn a pain concept, then apply it during a split squat, landing drill, or treadmill progression.
- Hands-on care with context: Dry needling, manual techniques, or myofascial work make more sense when you understand they can calm sensitivity and support movement, not "fix" a fragile body.
- Sport-specific transfer: A baseball athlete may work through rotational loading. A runner may pair education with gait analysis. A dancer may apply the same concepts during dance therapy and turnout-related control work.
- Return-to-sport decisions: Education supports stronger effort during hop testing, cutting progressions, and performance benchmarks because fear isn't driving the session.
The most effective education is timely, personal, and tied to a movement the athlete cares about.
For clinics trying to streamline the business side of rehab delivery while preserving one-on-one care, resources on specialized PT billing solutions can also be useful behind the scenes. Patients rarely think about that piece, but cleaner operations help protect time for actual treatment.
Metaphors athletes tend to remember
Here are a few analogies that tend to stick.
| Metaphor | What it means for the athlete |
|---|---|
| Smoke alarm | The system can sound even when the threat is lower than it feels. |
| Volume knob | Stress, poor sleep, fear, and past pain can turn sensitivity up. |
| Rusty hinge | Early movement may feel stiff and noisy, but that doesn't always mean damage. |
| Overprotective spotter | Your body may be trying to help, but with too much caution. |
| Practice before game speed | Confidence grows when you build load progressively, not when you skip straight to full intensity. |
Athletes who need lower-impact loading options sometimes benefit from tools discussed in this overview of advanced physical and aquatic therapy, especially when confidence in land-based loading is still developing.
Athlete Stories From Our South Shore Clinics
The soccer player after ACL surgery
You clear another phase after surgery, then the first pivot drill shows up and your body hits the brakes.
That was the pattern for a high school soccer player from Bridgewater after ACL surgery. Her range of motion was coming back. She showed up for strength work. On paper, recovery looked solid. But the second we introduced cutting and deceleration, she got stiff, shortened her stride, and moved like she was protecting the knee before the rep even started.
For an athlete, that can feel confusing. "If the graft is healing and I am getting stronger, why does my knee still feel so wrong?"
Part of the answer is that the body keeps a memory of threat. In sports terms, it is like a defender who keeps overplaying one side even after the scouting report changes. Early after surgery, protection makes sense. Later on, that same protective response can stay turned up longer than needed.
Once she understood that soreness, tension, and hesitation were not automatic signs of new damage, her practice sessions changed. We paired that education with hands-on sports PT, progressive deceleration drills, cutting mechanics, and return-to-sport testing. Her knee did not improve because we gave a speech. It improved because better understanding let her train with better quality and less guarding.
The runner with stubborn knee pain
A runner from the Plymouth area described the same frustrating pattern every week. His knee would start aching before he even found his pace.
That detail matters. If symptoms ramp up right away, especially after a few bad runs, the system may be reacting to expectation and sensitivity as much as load. Athletes often hear that and think it means the pain is "just in your head." That is not what we mean. The pain is real. The point is that real pain can come from a system that has become extra watchful.
A good sports analogy is a false start. The gun has not gone off, but the body is already reacting.
Once he had a clearer explanation for why stress, poor recovery, and past painful runs could turn the volume up, he stopped treating every ache as a sign that training was backfiring. We used graded mileage, strength work, and running form review alongside those conversations. His progress got more consistent because he was no longer changing the whole plan every time symptoms blipped upward.
Athletes recover better when they can sort out "this is sore" from "this is unsafe."
The dancer with hip pain that would not settle
A dancer from near Taunton came in frustrated because her hip felt unpredictable. One rehearsal would go fine. The next, familiar positions felt guarded from the start.
What helped was separating several things that had been getting lumped together. Pain. Tissue irritation. Fatigue. Load tolerance. Confidence. Those are related, but they are not identical.
That distinction matters a lot for athletes and post-surgical patients on the South Shore, especially in the early and middle phases of rehab. A sore response after a new drill can mean, "that was a new stress." It does not automatically mean, "something is going wrong." Once she understood that, we could build a dance-specific plan with clearer progressions instead of avoiding whole categories of movement.
None of these athletes improved from education alone. They improved because education changed how they interpreted symptoms, and that changed how they moved, loaded, and practiced in the clinic and outside it.
At PTU, that is how pain neuroscience education fits into rehab. It is woven into hands-on care, exercise progressions, sport-specific retraining, and the honest conversations that help an athlete stick with the process when recovery feels slower than expected.
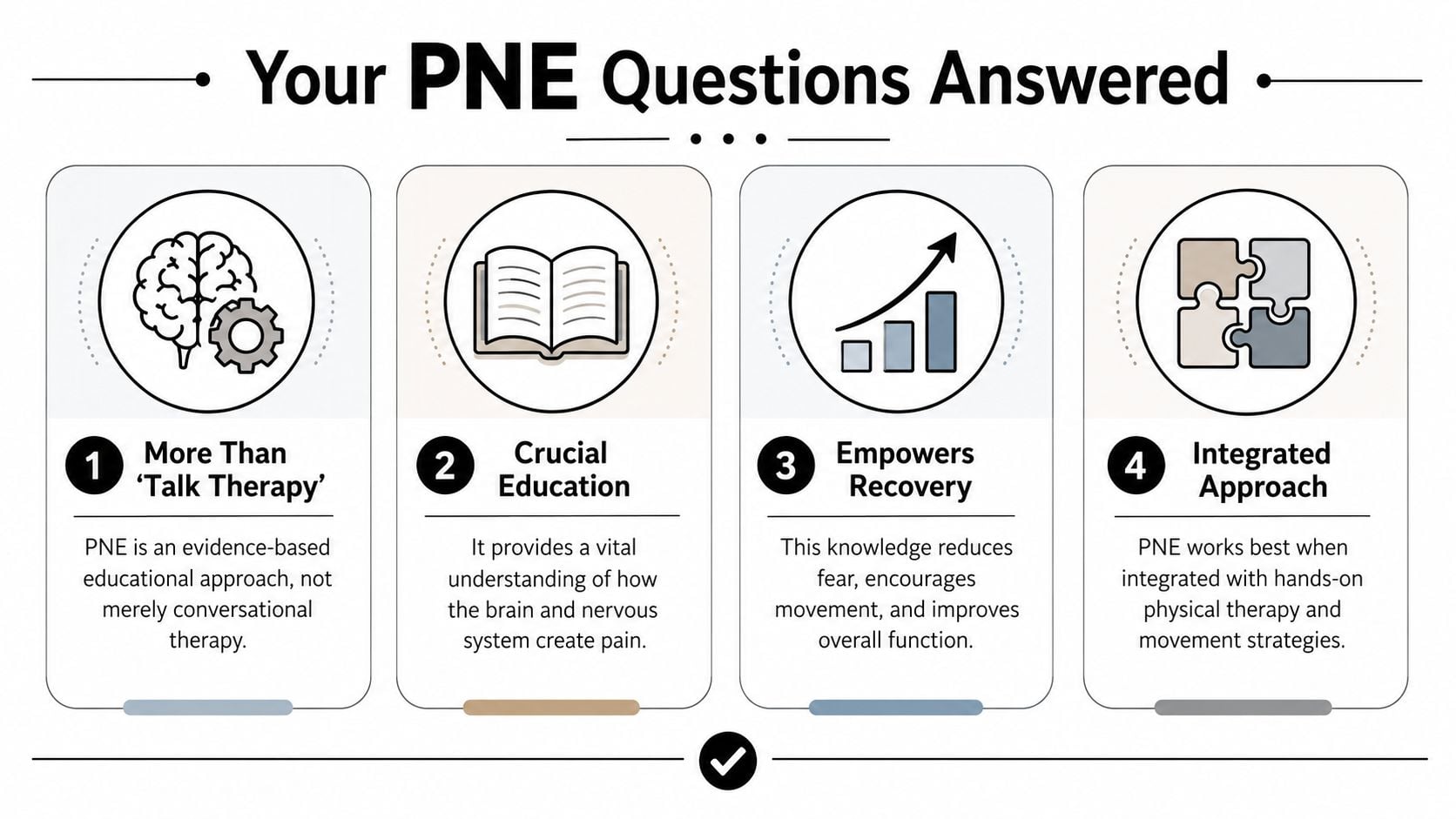
Your PNE Questions Answered
Is pain neuroscience education just talk therapy
No. It's education that helps you understand why pain behaves the way it does, so your physical rehab makes more sense.
For an ACL athlete, that can change how you interpret soreness during quad work, jogging progressions, and return-to-cutting drills. The point isn't to talk instead of train. The point is to train with better information.
Do I need a therapist for this
Usually, yes. Most athletes do better when a licensed PT explains the concepts in the context of their exam, stage of healing, and sport demands.
A handout or video can help, but they can't tell you whether your current symptoms fit expected recovery, whether your loading is appropriate, or how to progress safely.
How many sessions does it take
Pain education often starts with focused teaching, then gets reinforced over time during the rest of rehab.
That means you may cover the big concepts early, then revisit them when you hit sticking points like first jog, first jump, first lateral cut, or first full practice.
Can it help if I'm early after surgery
Yes, it can. As discussed earlier, this is an emerging area, but it's highly relevant for post-op and recently injured athletes who are trying to tell the difference between sensitivity and true danger.
Is this a replacement for medical care
No. If your symptoms are changing in a concerning way, you need an in-person evaluation. Pain neuroscience education is part of care, not a substitute for a proper physical therapy or medical assessment.
If you're an athlete, runner, dancer, or post-surgical patient in Bridgewater, Massachusetts, Buzzards Bay, Middleborough, or nearby South Shore towns like East Bridgewater, West Bridgewater, Raynham, Plymouth, and Taunton, you don't have to keep guessing what your pain means.
If pain is slowing your comeback, book an evaluation with Physical Therapy U. Our licensed DPTs provide athlete-centered sports physical therapy for ACL recovery, running injuries, dance medicine, return-to-sport testing, dry needling, and sport-specific rehab across Bridgewater, Buzzards Bay, and Middleborough.
{kind=link}