You're home after surgery. The nerve block is fading, the swelling is rising, and the prescription bottle on the counter suddenly feels like the whole recovery plan.
It isn't.
For athletes, runners, dancers, and active families across the South Shore of Massachusetts, post surgical pain management is part of performance rehab. If pain is poorly controlled, it becomes harder to sleep, harder to move, and harder to do the early work that protects range of motion, strength, and confidence. That matters whether you just had ACL reconstruction, shoulder surgery, meniscus repair, or another orthopedic procedure and want to get back to your sport without losing ground.
Table of Contents
- Your Post-Op Reality Check and Why Pain Isnt Just a Feeling
- The First 72 Hours Your Acute Pain Playbook
- Beyond the Pills Advanced Non-Drug Recovery Strategies
- Movement is Medicine Pacing Your Return to Action
- Opioid Stewardship Your Tapering Plan and Red Flags
- Start Your Comeback with PTU in Southeastern Mass
- Frequently Asked Questions About Post-Surgical Pain
Your Post-Op Reality Check and Why Pain Isnt Just a Feeling
The first mistake many athletes make is treating pain like something to “tough out.” That mindset works poorly after surgery. Pain changes how you move, how much you guard, how well you sleep, and whether you can tolerate the exercises that keep you from getting stiff.

A review published through the National Center for Biotechnology Information reported that 80% of patients who undergo surgery experience postoperative pain, and 88% of those patients describe it as moderate, severe, or extreme. The same review connects poor acute pain control with impaired physical function, poorer quality of life, slower recovery, longer opioid use, and higher costs of care.
For an athlete, that has a simple translation. If pain spikes, your knee doesn't bend well, your quad shuts down, your shoulder stays guarded, and therapy becomes something you endure instead of something you use to improve.
Why athletes should care about pain early
Pain after surgery isn't just a symptom. It's also a signal that can shape behavior.
- Less movement: You avoid positions that feel threatening, even when those positions are necessary for recovery.
- More swelling: Guarding and inactivity often go together, and that can make the joint feel even worse.
- Poorer sleep: When sleep drops off, tolerance for pain usually drops too.
- Delayed rehab participation: If you can't get comfortable enough to work on walking, range of motion, or muscle activation, the whole process slows down.
Pain control after surgery should support movement, not replace it.
Families in Bridgewater, Massachusetts, Plymouth, Taunton, East Bridgewater, and West Bridgewater often ask whether pain this intense is “normal.” Some pain is expected. What matters is whether there's a plan for it. A good plan reduces panic, improves consistency, and gives the athlete a way to stay engaged in recovery.
Not every painful issue after surgery is routine. If you've had abdominal surgery or have symptoms that don't match what your surgeon told you to expect, it can help to understand related complications such as the causes and diagnosis of abdominal abscess. That kind of symptom awareness matters because worsening pain without a clear reason deserves medical follow-up.
The First 72 Hours Your Acute Pain Playbook
The first three days are usually the least forgiving. Pain can rise quickly as anesthesia and nerve blocks wear off, and waiting until you're miserable is usually where people get into trouble.
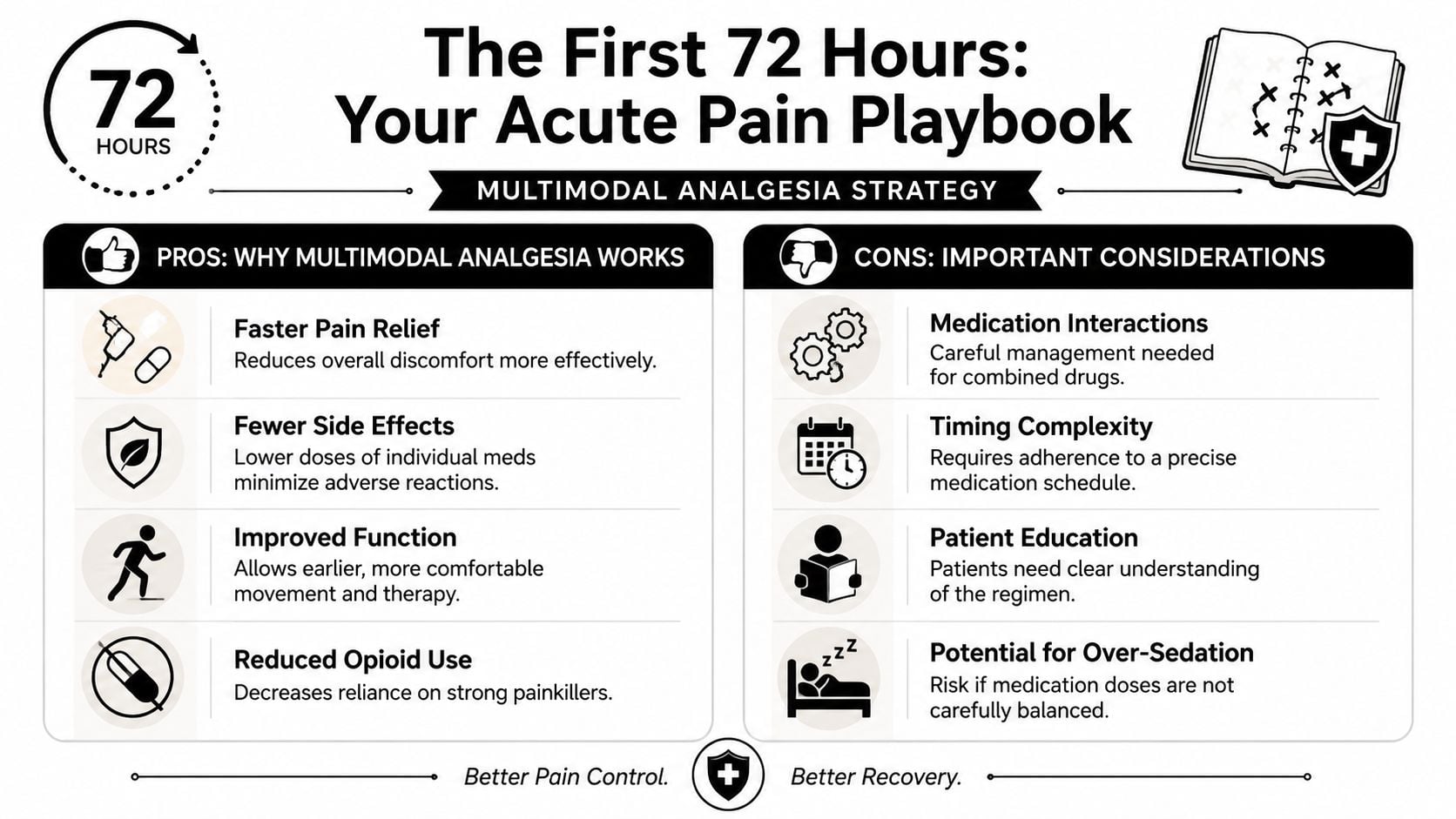
The most effective approach in this window is usually multimodal analgesia. In plain language, that means using more than one pain-control method so you're not relying on a single medication to do everything.
What multimodal analgesia actually means
According to StatPearls on postoperative pain control, adding acetaminophen or NSAIDs reduces opioid consumption and improves pain control compared with opioids alone. The same source notes that perioperative NSAIDs and COX-2 inhibitors can reduce IV morphine use by about 10 mg.
That matters because opioid-only strategies often create a bad trade. You may blunt pain, but you can also end up sedated, nauseated, constipated, or mentally foggy. None of that helps an athlete get up, eat, hydrate, and begin basic movement.
A practical post-op plan often includes a few layers:
- Scheduled non-opioid medication: This is commonly the foundation, assuming your surgeon says it's safe for you.
- Opioids only when needed: These are often most useful for breakthrough pain, especially at night or right before a difficult stretch of the day.
- Ice, elevation, and compression: These help when swelling is driving the pain.
- Early gentle movement: Not heavy exercise. Just enough motion to keep the system from locking down.
Later in the first days, this overview can help patients and parents see the logic visually:
A simple first-days routine
The exact medication plan has to come from your surgeon, because procedure type, age, medical history, and restrictions all matter. But the structure should usually look organized, not reactive.
Here's the pattern I want athletes to understand:
- Start with the surgeon's written schedule. Don't guess. Don't combine medications casually.
- Use non-opioid meds on time if they're prescribed that way. The whole point is to stay ahead of the pain curve.
- Reserve stronger medication for pain that breaks through despite the base plan.
- Match medication timing to sleep and movement. If a walk to the bathroom, home exercise, or first PT visit is coming, poor timing can make everything harder.
- Track your response. If pain stays uncontrolled, call the surgeon's office instead of just taking more on your own.
Practical rule: The first 72 hours usually go better when you follow a schedule than when you chase pain after it spikes.
A few mistakes show up over and over:
- Waiting too long: Athletes try to be “good” and hold off until pain is severe.
- Taking meds but not moving at all: Pain relief should help you do something useful.
- Moving too aggressively because the medication masks symptoms: Feeling better for a few hours doesn't mean the tissue is ready for more load.
- Ignoring hydration, food, and sleep: Medication tolerance usually gets worse when those basics fall apart.
If you're a high school athlete in Bridgewater or West Bridgewater recovering from ACL surgery, shoulder stabilization, or meniscus repair, the first win isn't heroic effort. It's predictable control. Better pain control early often means a calmer knee, a less guarded shoulder, and a smoother handoff into rehab.
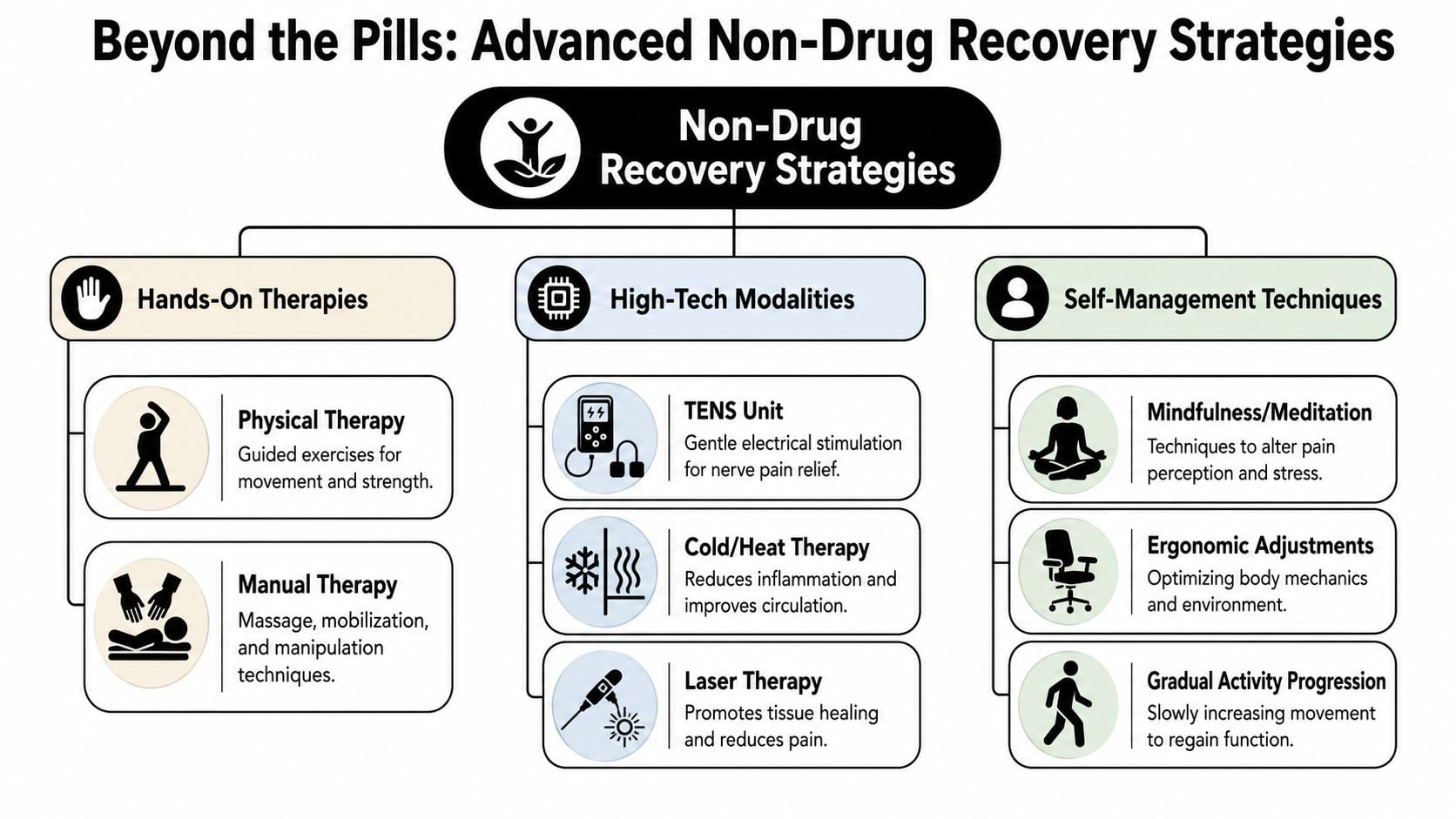
Beyond the Pills Advanced Non-Drug Recovery Strategies
Medication matters. It's just not the whole picture.
Once the immediate surgical pain begins to settle, the focus shifts toward swelling control, tissue irritation, muscle guarding, and your ability to tolerate rehab. Non-drug strategies often make the difference here between feeling stuck and starting to move like an athlete again.
A project on multimodal post-surgical pain control found that after implementation, patient-reported pain scores fell from 4.8 to 2.82 out of 10, and opioid use decreased by 72%, with high patient satisfaction, as reported in this multimodal analgesia project summary. The useful takeaway is not that one trick fixed everything. It's that combining tools worked better than leaning on one category alone.
What helps at home
Some of the best pain-management tools are low-tech and repeatable.
- Ice with a purpose: Use it to calm swelling and sensitivity, especially after exercises or periods of being upright.
- Proper limb positioning: For a knee or ankle, this means getting the limb supported well, beyond merely reclining a little on the couch.
- Compression: A post-op wrap, sleeve, or surgeon-approved compression option can help when the joint feels full and tight.
- Position changes: Staying in one position too long usually backfires. Small changes can reduce stiffness and muscle guarding.
- Breathing and downshifting: Short, steady breathing can lower the threat response that amplifies pain.
These aren't flashy. They work because they're repeatable and because they reduce the inputs that make pain feel bigger than the tissue irritation alone.
Where skilled rehab changes the picture
The right clinical tools can help when pain is being driven by guarding, swelling, stiffness, and overload in the surrounding tissues.
In athlete-centered rehab, common add-ons include:
- Manual therapy and myofascial work: Helpful when surrounding muscles lock down and start protecting the area too aggressively.
- Dry needling: In the right patient and at the right stage, this can reduce muscle guarding around the surgical region and make movement feel less threatening.
- Laser therapy: Some clinics use it to calm irritated tissue and support recovery. If you want a deeper explanation of that approach, this overview of laser therapy for inflammation is useful.
- Compression recovery systems: Athletes often respond well to structured compression sessions when swelling and heaviness are limiting movement tolerance.
A good non-drug plan should make exercise easier to do, not become a substitute for exercise.
Advanced sports physical therapy stands apart from generic rehab. A runner may need swelling control plus gait reintroduction. A dancer may need pain relief without losing turnout control. An ACL athlete may need quad activation, patellar mobility, and confidence restoring at the same time.
The point isn't to throw every modality at the problem. The point is to choose the few that match the current barrier. When the barrier changes, the plan should change too.
Movement is Medicine Pacing Your Return to Action
Pain control earns its value when it helps you move better.
That's the shift many athletes need to hear. The goal isn't to win a pain-score contest. The goal is to restore motion, rebuild tolerance, and start loading the right tissues at the right time.
A recent review on acute postoperative pain noted that severe acute pain is common, affecting up to 40% of patients on the first day after surgery, and that successful rehab depends on pairing pain assessment with functional metrics rather than pain intensity alone, as outlined in this review of acute postoperative pain management. That means we care about your pain, but we also care whether you can sleep, walk, bend, lift your leg, and tolerate the next phase of rehab.
What early movement should feel like
Early movement should be controlled, specific, and a little boring. That's usually a good sign.
For most athletes, appropriate early rehab includes some combination of:
- Gentle range of motion work: Enough to prevent stiffness without provoking a major flare.
- Muscle activation drills: Think quad sets after knee surgery or scapular control work after shoulder surgery.
- Walking mechanics: Not distance for the sake of distance. Better quality first.
- Swelling-sensitive loading: If the joint gets dramatically more swollen after a session, the dose was probably too high.
What doesn't work well is the all-or-nothing approach. Some athletes do too little because they're afraid. Others do too much because they're impatient. Both can stall progress.
If function improves but pain stays a little present, that can still be a solid rehab day.
Examples after common sports surgeries
Take an ACL athlete in South Shore Massachusetts. Early on, the priorities are often getting the knee to calm down, restoring extension, improving flexion gradually, waking up the quad, and walking more normally. If pain is too high, each of those tasks gets harder.
A shoulder athlete often faces a different problem. Pain creates guarding, guarding limits range, and limited range makes basic exercises feel worse than they should. In that case, pacing, support positions, and carefully chosen mobility work matter just as much as medication.
For knee patients who want a practical look at progression, these knee replacement recovery exercises show the bigger principle well. Start with what the tissue can tolerate, then build from there.
In sports rehab, we also have to think beyond the first month. Runners need a return-to-run progression. Dancers need control in end-range positions. Field and court athletes need deceleration, cutting, and eventually return-to-sport testing. Pain management is the opening chapter, not the whole story.
Opioid Stewardship Your Tapering Plan and Red Flags
Families usually want a straight answer about opioids. Here it is.
They can be appropriate after surgery, especially when pain is severe and short-term control matters for sleep, early mobility, and basic recovery. But they work best as one tool inside a broader plan, not as the foundation of the plan.
Recent clinical coverage on opioid-free and opioid-sparing care emphasizes that the evidence supports individualized planning, not a one-size-fits-all no-opioid rule, as discussed in this review of post-surgical pain treatment without opioids. That's exactly how athletes and parents should think about it.
When opioids still have a role
A short course may make sense when:
- Pain is breaking through the rest of the plan
- Sleep is falling apart because of pain
- The first days after surgery are too intense to manage with non-opioid options alone
- The surgeon specifically expects a higher-pain recovery
The tapering idea is simple. As pain becomes more predictable and function improves, you lean more on the base plan and less on rescue medication.
A practical framework often looks like this:
- First step: Stop taking opioids on an automatic schedule if you've been doing that and your surgeon clears the change.
- Next: Use them only for breakthrough pain or the hardest part of the day.
- Then: Drop one use at a time, usually starting with the least necessary dose.
- Finally: Stay with the non-opioid and recovery supports that are still helping.
If your medication list includes more than one sedating drug, ask questions early. Families who want a plain-language overview of combined-medication concerns may find this resource on gabapentin and oxycodone risks helpful.
Red flags that need a call right away
Not all pain patterns are routine.
Call your surgeon promptly if you have:
- Pain that is suddenly escalating instead of gradually settling
- Fever or chills
- Calf pain, unusual calf tenderness, or major swelling that seems out of proportion
- Drainage, redness, or a wound that looks worse instead of better
- Shortness of breath, chest symptoms, or fainting
- Sedation, confusion, or medication side effects that feel unsafe
- Pain so uncontrolled that you can't sleep, move, or follow the basic recovery plan
The taper should feel deliberate, not dramatic. If pain is staying high longer than expected, the answer isn't always “take more” or “stop everything.” Sometimes the issue is swelling, poor timing, overactivity, constipation, anxiety, or a complication that needs the surgeon's input.
Start Your Comeback with PTU in Southeastern Mass
Good post surgical pain management should help you do three things. Calm the early chaos, restore movement, and build toward confident return to sport.
That's the model at Physical Therapy U. As an athlete-centered sports physical therapy clinic, PTU pairs evidence-based rehab with the tools active people need after surgery, including dry needling, myofascial work, recovery sessions with NormaTec compression, running gait analysis, dance therapy, sport-specific training, and return-to-sport testing. For some patients who need broader support around pain and substance-use concerns, outside education on strategies for managing addiction and pain can also be valuable alongside medical care.
If you're looking for more advanced rehab options, PTU also offers advanced physical and aquatic therapy to help patients keep progressing when standard exercise alone isn't enough.
With locations in Bridgewater, Massachusetts, Buzzards Bay, and Middleborough, PTU serves athletes and active families across Southeastern Massachusetts, including Plymouth, Raynham, Taunton, East Bridgewater, and West Bridgewater. If you want a plan that goes beyond “rest and take your meds,” book an evaluation and start your comeback with a team built around sports rehab.
Frequently Asked Questions About Post-Surgical Pain
How much pain is normal after surgery
Some pain is expected. What matters more than the exact number is the trend. The pain should become more manageable, less reactive, and less disruptive to sleep, movement, and daily tasks as recovery progresses.
When should I worry that acute pain is turning into a bigger problem
One of the main concerns after surgery is the transition from acute pain to chronic postsurgical pain. Guidance from the American Society of Regional Anesthesia and Pain Medicine notes that standard acute pain treatments have limited evidence for preventing that transition, while strategies such as regional anesthesia, continuous peripheral nerve blocks, and some newer neuromodulation approaches may help. It also reinforces the need for close follow-up so the rehab team can monitor the pain trajectory over time in this discussion of acute pain management to prevent chronic postsurgical pain.
When can dry needling be used after surgery
That depends on the procedure, the tissue being treated, incision healing, surgeon preferences, and the reason for using it. Dry needling is not usually the first thing done immediately after surgery. It's often considered later when muscle guarding, protective spasm, or surrounding tissue overload is limiting progress.
When should I stop all pain medication
There isn't one universal day. Most athletes taper off stronger medication first, then continue only what is still clearly helpful and approved by the surgeon. If you're taking medication but still not functioning better, it's time to reassess the plan rather than just extending it.
I was told to go to PT. What should I expect at the first visit
Expect a focused conversation about your surgery, current symptoms, precautions, swelling, sleep, mobility, and sport goals. A licensed physical therapist should also look at function, not just pain. That includes how you walk, how you tolerate position changes, what motion is available, and what the next safe step should be.
Can pain management affect return to sport
Yes. Early pain control shapes your ability to restore range of motion, activate the right muscles, tolerate loading, and stay consistent with rehab. For athletes, that influences the entire return-to-sport timeline, even though pain relief itself is never the final goal.
If you're recovering from surgery and want a sports-focused plan that matches your goals, book with Physical Therapy U. Our licensed DPTs help athletes and active adults across Bridgewater, Buzzards Bay, and Middleborough move from pain control to real performance recovery.
{kind=link}