You're probably reading this in one of two moments. You've just had ACL surgery and your knee feels swollen, stiff, and foreign. Or surgery is coming up, and you're trying to understand what recovery will look like when the hospital handout runs out of detail.
For athletes, runners, and dancers, what to expect after ACL surgery goes far beyond getting the incision to heal. Walking around the house and getting back to cutting, sprinting, jumping, landing, or performing aren't the same thing. That gap is where a lot of frustration shows up, especially when the knee starts to feel better before the body is fully ready.
At Physical Therapy U, our licensed DPTs work with athletes across Southeastern Massachusetts, including Bridgewater, Buzzards Bay, Middleborough, Plymouth, Taunton, Raynham, East Bridgewater, and West Bridgewater. The pattern is familiar. The early phase feels slow. The middle phase feels more encouraging. The late phase is where discipline matters most, because that's when athletes are tempted to test the knee before they've earned it.
Table of Contents
- An Athlete's Roadmap to ACL Recovery
- The First 48 Hours Navigating Immediate Post-Op
- Weeks 1-6 Building Your Recovery Foundation
- Months 2-4 Progressing Strength and Function
- Months 5-9 Plus The Athlete's Return-to-Sport Journey
- ACL Recovery Red Flags What Is Not Normal
- Your ACL Recovery FAQs
- Q. When can I shower after surgery?
- Q. When can I drive again?
- Q. How long will I wear the brace?
- Q. What's the best sleeping position?
- Q. Will I be able to kneel again?
- Q. When can I start running?
- Q. Why does my knee feel stiff even when it's getting stronger?
- Q. Do I need return-to-sport testing if I feel ready?
- Your Next Step in ACL Recovery on the South Shore
An Athlete's Roadmap to ACL Recovery
The biggest mindset shift after ACL surgery is this: your recovery happens in phases, not in one straight line. Early on, the wins are simple. Less swelling. Better sleep. A more normal walk. Later, the goals become much more demanding, because sport asks more of your knee than everyday life ever will.
That's why the timeline athletes hear from friends is often misleading. According to Mass General Brigham's ACL reconstruction guidance, most patients can resume routine activities within weeks to a few months, but return to sports commonly takes about 9–12 months. That lag exists because graft healing is staged, and neuromuscular recovery doesn't keep pace with pain relief or basic walking.
Practical rule: If your knee feels “pretty good,” that's encouraging. It is not the same thing as being ready to compete.
Athletes around the South Shore often struggle most during the middle stretch. The crutches are gone. The incision looks better. Friends assume you're almost back. But considerable work is still ahead. Strength has to come back. Landing mechanics have to clean up. Confidence has to return without turning into impatience.
A good recovery plan accounts for both the tissue and the athlete. It respects healing, but it also trains toward performance. That means objective milestones, progressive loading, movement quality, and eventually sport-specific drills that fit your actual demands, whether that's soccer, basketball, football, lacrosse, dance, or running.
If you want a deeper conversation about the sport side of this injury, the ABCs of the ACL with Dr. Eric Rightmire podcast episode is a useful listen.
The First 48 Hours Navigating Immediate Post-Op
You get home after surgery, the nerve block starts wearing off, and the knee feels heavier and stiffer by the hour. Athletes often assume they should grit their teeth and try to do more. In the first 48 hours, that mindset usually creates more swelling, more pain, and a rougher start to rehab.

The first day at home
Treat the first day like setup, not training. Keep water, medications, your phone charger, ice or your cooling device, and anything you use often within arm's reach. If a family member or teammate is helping, they should know your medication schedule, brace instructions, and how you're supposed to get up and down safely.
Early priorities are straightforward. Control swelling, protect the graft and incision, and keep blood moving. Guidance from the University of Washington Orthopaedics ACL aftercare instructions supports keeping the leg raised above heart level when resting and doing frequent ankle pumps to support circulation in the first few days.
One practical point matters here. Use the help you have. The athlete who tries to hop to the bathroom alone at 2 a.m. is usually the same athlete who irritates the knee, misses a dose of medication, or scares themselves with a near fall.
What helps in the first 48 hours
Pain control matters, but so does pacing. The goal is a calm knee, not a heroic effort.
- Raise the leg well: Rest with the leg supported so swelling has a chance to settle. Lying flat with the knee hanging around all day usually leaves the joint more irritable.
- Do ankle pumps regularly: They seem minor, but they help circulation and give you a simple task you can do often without stressing the knee.
- Use crutches as instructed: Protected walking is better than limping through short trips and reinforcing bad mechanics.
- Follow incision and dressing instructions exactly: Keep the wound clean and dry. Do not improvise with wraps, ointments, or shower shortcuts your surgeon did not approve.
- Take prescribed medication on schedule early on: Staying ahead of pain is often easier than trying to calm it down once it spikes.
- Keep activity boring: Short bathroom trips, position changes, and basic home mobility are enough right now. If you are used to hard training, this is a good time to read about return-to-running strength and movement work for runners, not test your limits on day one.
The best first 48 hours are usually quiet, controlled, and uneventful.
One common early mistake
Putting a pillow directly under the knee feels good in the moment. I still have to coach athletes out of this all the time. It leaves the knee resting in flexion, and that can make it harder to regain full extension once the initial pain settles down.
Support the whole leg instead, with the knee allowed to straighten rather than sag into a bent position. Comfort matters, but early positioning has consequences for walking, quad activation, and the pace of the next phase.
Recovery also depends on the basics athletes tend to overlook when they are focused on the surgical knee alone. Hydration, protein intake, sleep, and simple strategies to optimize muscle recovery can make those first few days more manageable while your body deals with the stress of surgery.
Weeks 1-6 Building Your Recovery Foundation
By the end of week one, many athletes have the same reaction. The incision looks fine, the pain is more manageable, and they assume the hard part is over. In reality, this is the phase that often sets up the rest of the recovery. If swelling stays high, the knee will not move well. If full extension is missing, walking gets awkward fast. If the quad stays inhibited, everything after this gets harder.

What matters most early
In our Southeastern Massachusetts clinics, weeks 1 through 6 are about three things. Get the swelling down. Get the knee fully straight. Get the quadriceps working again.
Athletes usually want to chase bending first because it feels like visible progress. I get that. But a knee that bends well and will not fully straighten is a problem. Extension affects gait, standing tolerance, quad recruitment, and how cleanly you can move into the next phase.
Quad inhibition is the other big issue. The muscle has not disappeared, but after surgery the brain often struggles to recruit it. That is why a straight leg raise or a quad set can feel harder than it looks. Early rehab is not impressive to watch, but it matters.
What good progress usually looks like
Good early rehab looks controlled, repeatable, and a little boring. Athletes who do well in this phase usually stop trying to win the day and start stacking solid days together.
A typical plan may include:
- Quad sets: Used to restore a clean contraction and reduce the lag that often shows up after surgery.
- Heel slides: Helpful for regaining motion without cranking into pain.
- Heel prop or other supported extension work: Used to regain full straightening so walking mechanics do not stay stuck.
- Patellar mobility and hands-on treatment: Useful when stiffness around the kneecap is limiting motion or comfort.
- Gait training: Crutches often stay longer than athletes expect if the knee is swollen, bent, or poorly controlled.
- Stationary bike later in the phase: Often added once motion allows a smooth pedal stroke.
The trade-off in this window is simple. Push too hard and the knee gets more reactive. Do too little and stiffness and weakness settle in. The right program challenges the knee without stirring it up for the next 24 hours.
What commonly slows athletes down
A few mistakes show up over and over.
- Letting the knee rest in slight flexion for hours at a time: This still happens at home on couches, recliners, and car rides.
- Walking with a bent knee because it feels safer: It may feel protective, but it reinforces poor mechanics and keeps the quad quiet.
- Chasing range aggressively: More force is not better if the joint responds with extra swelling.
- Adding twisting, pivoting, or heavier open-chain quad work before the knee is ready: Tissue healing and graft choice matter here, so progression has to match the surgeon's guidance and the athlete's presentation.
At Physical Therapy U, we also pay attention to the athlete, not just the joint. Sleep quality, hydration, protein intake, and day-to-day soreness all affect what the knee gives you in the clinic. If you want practical ways to optimize muscle recovery, that can support the work you are already doing in rehab.
For runners, this phase is also a good time to clean up the pieces above and below the knee that will matter later. Our guide to physical therapy exercises for runners covers hip strength, control, and movement habits that become important once running is back on the table.
The standard we use in clinic
I do not judge this phase by how hard the exercises look. I judge it by whether the knee is calming down and whether movement quality is improving.
By the end of this foundation phase, the athlete should be moving toward a quieter knee, cleaner quad activation, better walking mechanics, and more confidence with basic daily tasks. Those are not glamorous wins. They are the wins that make later strength and return-to-sport testing possible.
Months 2-4 Progressing Strength and Function
This phase usually feels more productive. The knee is less reactive. Daily movement is easier. You can finally train instead of just managing symptoms. That said, this is still a build phase, not a return-to-sport phase.
What training starts to look like
Exercise selection becomes more functional now. Athletes often transition from isolated activation toward controlled strength work through the hips, quads, hamstrings, and calf, plus balance and position control.
A typical progression may include:
- Stationary bike work: Useful for motion, blood flow, and gradually building tolerance.
- Leg press within appropriate range: A common way to load the lower body without jumping too far ahead.
- Step-ups and controlled split-stance work: These expose side-to-side asymmetries quickly.
- Single-leg balance drills: Helpful for proprioception and positional control.
- Core and hip strengthening: Often overlooked by patients, but critical for knee mechanics.
This is also where athletes start to learn the difference between exercise and rehab progression. More weight isn't always better. Better control is better. If the knee swells more after a session, if mechanics fall apart, or if the unaffected leg is doing all the work, the program needs adjustment.
A strong-looking compensation is still a compensation.
What athletes usually notice in daily life
The wins in this phase are practical. Stairs feel less awkward. Walking looks more normal. Standing for longer periods is easier. You start trusting the leg again during basic tasks.
But there are trade-offs. The knee may still feel stiff after sitting. Swelling may come and go based on load. One hard session can make the next day feel like a step backward. That's normal if the response is mild and settles. It's not a sign that the rehab isn't working.
This stretch also benefits from structure outside formal PT. A smart lifting progression and performance mindset can help, as long as it respects healing. That's where a plan like this strength and conditioning program for athletes fits well. It reinforces that strength work isn't separate from rehab. For an athlete, it becomes the bridge back to performance.
Months 5-9 Plus The Athlete's Return-to-Sport Journey
Now, the conversation changes. The question stops being “How's your knee doing?” and becomes “What can your body prove?”

Why feeling good is not enough
A lot of athletes feel dramatically better before they're fully ready for cutting and pivoting. That mismatch is one of the biggest risks in ACL rehab. Hospital for Special Surgery emphasizes in its ACL surgery recovery guidance that time alone is a poor clearance metric, and many athletes who feel normal by the middle months still aren't ready for cutting, jumping, or contact demands.
The most important return-to-sport timing point comes from Johns Hopkins Medicine's ACL reconstruction overview. It notes that returning to cutting and pivoting sports before 9 months post-surgery is associated with substantially higher re-injury risk, and that for each month an athlete delays return past 6 months, up to 9 months, re-injury rate can decrease by as much as 51%.
That doesn't mean every athlete should just sit and wait. It means the later phase should be earned with testing, progression, and proof.
Here's a short demo that shows the performance side of the process:
What return-to-sport testing should include
A real return-to-sport process should look more like screening for competition than graduating from basic rehab. It should include objective data and movement analysis, not just a date on the calendar.
At a sports physical therapy clinic, that often means:
- Strength testing: Looking for meaningful side-to-side symmetry, especially in the quadriceps.
- Hop testing: Single-leg hop variations can reveal power deficits and poor shock absorption.
- Landing and cutting analysis: Video helps catch knee valgus, trunk shift, hesitation, and poor deceleration mechanics.
- Running assessment: For runners, gait analysis helps identify compensations that may not show up in a simple strength test.
- Sport-specific movement progressions: A soccer player, basketball guard, dancer, and distance runner do not need the same exposure plan.
- Psychological readiness: Athletes need confidence, but they also need trust in the limb under speed, fatigue, and decision-making.
For runners building back toward endurance events, outside education can also help frame the bigger conditioning picture. A practical marathon training essentials guide can be useful once running is appropriate and the rehab team has already cleared that direction.
For dancers, this stage usually requires even more precision than patients expect. Releve, turnout control, repeated landings, and choreography demands expose subtle deficits quickly. For field and court athletes, the issue is usually deceleration and reactive change of direction. Both groups need more than “it doesn't hurt.”
ACL Recovery Red Flags What Is Not Normal
Most ACL recoveries are straightforward. Some discomfort, bruising, warmth, and swelling are expected. The key is knowing the difference between a normal healing response and a symptom that needs urgent attention.
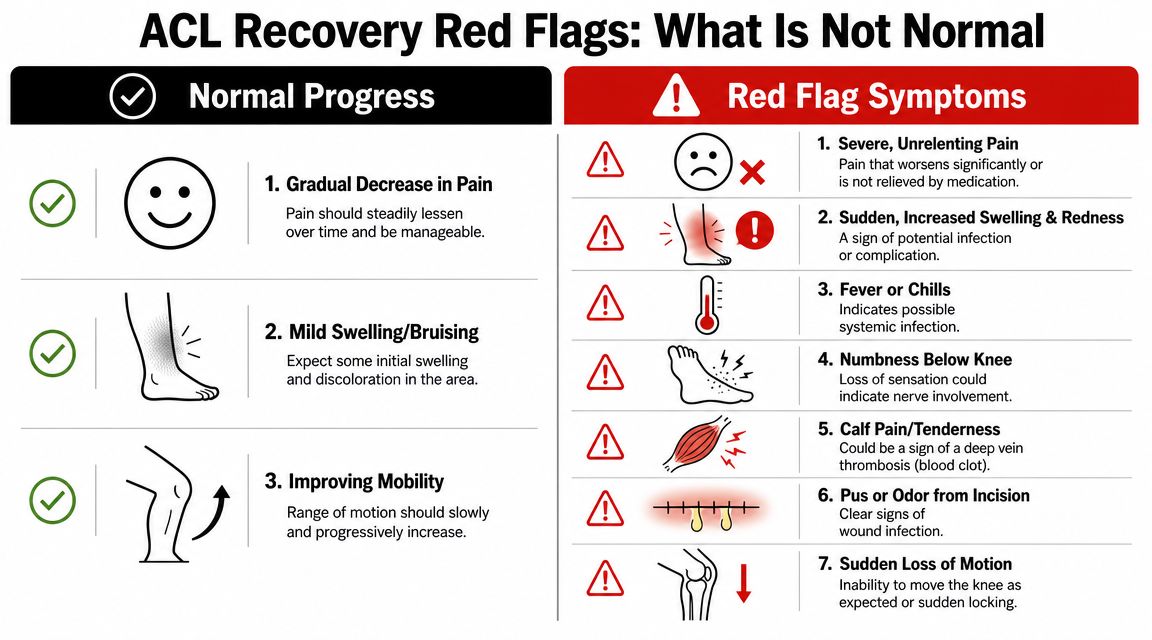
Normal early symptoms versus warning signs
The red flags most worth remembering come from this patient education discussion on post-op warning signs. Patients should be alert for calf pain or swelling, shortness of breath or chest pain, or fever with worsening knee redness or swelling. Those complications are described there as rare but serious and requiring immediate medical attention.
Here's the practical version:
| Symptom | What it may mean | What to do |
|---|---|---|
| Mild swelling and bruising | Common early post-op response | Monitor it and follow your prescribed care plan |
| Warmth around the knee | Often part of healing | Watch the trend, especially if other symptoms appear |
| Calf pain or marked calf swelling | Possible blood clot | Contact your surgeon immediately or seek urgent medical care |
| Shortness of breath or chest pain | Possible pulmonary embolism | Go to the nearest emergency department now |
| Fever with worsening redness or swelling at the knee | Possible infection | Contact your surgeon right away |
| Sudden dramatic worsening | Could reflect a complication | Don't wait for your next PT visit to mention it |
If a symptom feels out of proportion or changes quickly, treat that as a reason to call.
Athletes sometimes minimize symptoms because they don't want to overreact. After surgery, that instinct can be unhelpful. If you're unsure whether something is normal, ask the surgical team or your licensed physical therapist. It's much better to check early than to explain later why you waited.
Your ACL Recovery FAQs
Q. When can I shower after surgery?
That depends on your surgeon's incision and dressing instructions. Follow those exactly. Don't guess based on a friend's experience, because closure method and post-op protocol can differ.
Q. When can I drive again?
Driving depends on which leg had surgery, whether you're off medications that impair reaction time, and whether you can safely brake without hesitation. This is a surgeon-cleared decision, not a milestone to self-test in a parking lot.
Q. How long will I wear the brace?
Brace use varies by surgeon preference, graft choice, and any added procedures. Some athletes are out of it sooner, while others stay in it longer. The important part is not comparing your timeline to someone else's.
Q. What's the best sleeping position?
Most patients do best on their back at first with the leg supported in a way that doesn't keep the knee bent. Comfort matters, but avoid setups that leave the knee resting in flexion for hours.
Q. Will I be able to kneel again?
Many people can kneel again, but it may feel uncomfortable for a while, especially depending on the surgical site and local sensitivity. Tolerance usually improves gradually with healing, desensitization, and exposure.
Q. When can I start running?
Running is usually introduced only after strength, swelling response, range of motion, and single-leg control are good enough to handle impact. Athletes often want this step early, but starting too soon usually exposes deficits you can't outrun.
Q. Why does my knee feel stiff even when it's getting stronger?
That's common. Strength and tissue irritability don't always improve at the same pace. A knee can test stronger and still feel tight after sitting, after training, or first thing in the morning.
Q. Do I need return-to-sport testing if I feel ready?
Yes. Feeling ready matters, but it's incomplete. Athletes should have objective testing before they return to higher-risk sport demands, especially if cutting, pivoting, jumping, or contact are involved.
Your Next Step in ACL Recovery on the South Shore
A strong ACL recovery isn't just about getting through rehab visits. It's about progressing from surgery to full performance with a plan that respects healing, restores movement quality, and reduces avoidable re-injury risk.
For athletes in Bridgewater, Massachusetts, Buzzards Bay, Middleborough, and across the South Shore Massachusetts region, the biggest advantage is working with a sports physical therapist who understands your actual goal. Not just walking without pain, but returning to your sport with confidence and objective readiness. That may include sport-specific training, dry needling, running gait analysis, dance therapy, and return-to-sport testing based on how you move, not just how many months have passed.
If you're recovering from ACL surgery and want athlete-centered guidance in Southeastern Massachusetts, book an evaluation with Physical Therapy U. Our team serves athletes and active adults from Bridgewater, Buzzards Bay, Middleborough, Plymouth, Taunton, Raynham, and nearby communities with sports rehab built around strength, movement quality, and safe return to play.
{kind=link}