You hear a pop cutting to the ball in a soccer match. Or you land from a dance turn, catch yourself with your hand, and now your wrist won't tolerate weight. Or maybe you're a runner in South Shore Massachusetts who kept pushing through “just tightness” until a normal training day became a limp home.
At that point, most athletes and parents ask the same question. Do we need physical therapy or occupational therapy? The two can sound interchangeable, but they aren't. For an athlete trying to get back to practice, performance, and confidence, the difference matters.
This guide is written from a sports rehab perspective for injured athletes, active adults, dancers, and post-surgical patients. If you're in Bridgewater, Massachusetts, or coming from Plymouth, Taunton, East Bridgewater, West Bridgewater, Raynham, Buzzards Bay, or Middleborough, this is the practical version of physical therapy vs occupational therapy you need.
Table of Contents
- Your Comeback Starts Here But with Whom?
- The Foundations Two Disciplines One Goal
- A Side by Side Comparison PT vs OT
- What Conditions Do PTs and OTs Treat
- Real World Scenarios for Athletes
- Making the Right Choice for Your Recovery
- Your Integrated Recovery Team at Physical Therapy U
- Frequently Asked Questions About PT and OT
Your Comeback Starts Here But with Whom?
A high school athlete usually doesn't care about professional labels. They care about one thing. How do I get back in the game?
That's why this question gets tricky. A torn ACL after basketball, a jammed finger that never settled down after volleyball, and shoulder pain during throwing can all feel like “I need rehab.” True. But the best rehab path depends on what's limiting you.
The first question isn't the diagnosis
A diagnosis matters, but in real practice the better starting point is often your functional bottleneck. Can you not squat, cut, sprint, land, and absorb force? That points more toward physical therapy. Can you move the arm, but still can't grip a bat, button a shirt, handle schoolwork, or manage sport equipment with control? That may point more toward occupational therapy.
Practical rule: Don't ask only, “What injury do I have?” Ask, “What can't I do right now that I need to do?”
For athletes and parents, confusion usually comes from the names. “Physical therapy” sounds broad, and “occupational therapy” sounds like it only applies to jobs. In reality, occupation means meaningful activity. For a student-athlete, that can include school tasks, self-care, hand use, sport-specific task performance, and return to normal daily life after injury or surgery.
What matters for an athlete
If your goal is return to sport, you need the provider whose plan matches the problem in front of you.
- If the barrier is movement capacity: Think pain, stiffness, weakness, balance loss, reduced mobility, poor loading tolerance, or loss of running and jumping mechanics.
- If the barrier is task performance: Think gripping, writing, taping, dressing, hand coordination, stick handling, ball handling, or using the arm and hand effectively in daily life and sport.
- If both are true: You may need both disciplines involved.
That's where a lot of generic explanations fall short. Athletes don't need a textbook distinction. They need a clear answer about who helps with the exact thing that's blocking their comeback.
The Foundations Two Disciplines One Goal
Both professions help people function better, but they were built from different starting points. That history still shapes what each one does best today.
Why their history still matters
Occupational therapy was organized nationally in 1917 and grew from the “moral treatment” and arts-and-crafts movements, while physical therapy was formalized in the United States with the creation of the American Women's Physical Therapeutic Association in 1921 to rehabilitate injured soldiers, as outlined by MCPHS on occupational therapy vs physical therapy.
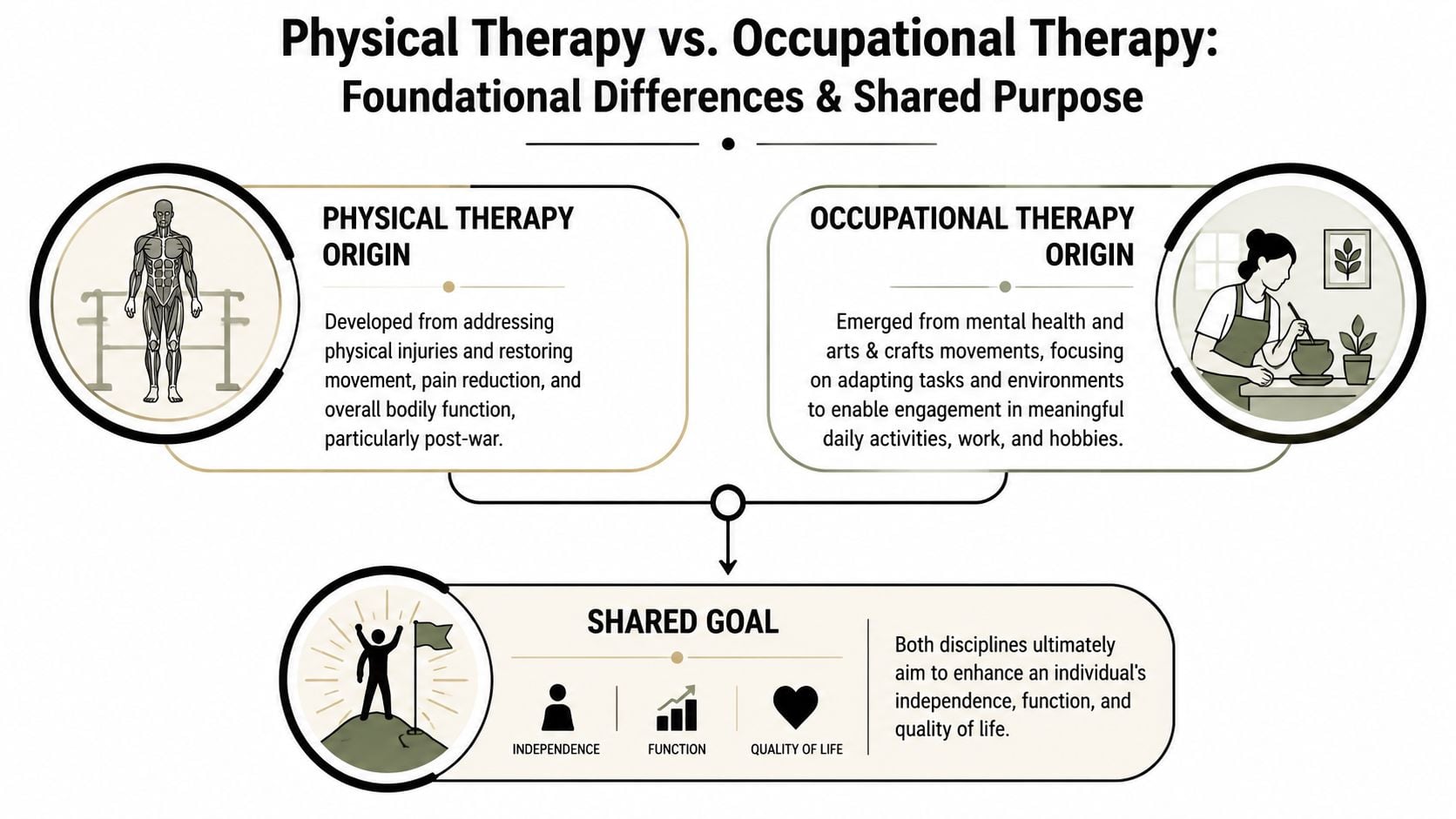
That means PT grew around restoring the body's movement system. OT grew around helping people participate in meaningful activities. Those ideas still hold up in a sports clinic.
A PT is usually asking questions like these:
- How does the knee load
- Can the shoulder move well enough
- Is the athlete producing force well
- Can they decelerate, cut, land, and tolerate sport demands
An OT is usually asking something different:
- Can the patient use the hand effectively
- Can they perform daily tasks without compensating poorly
- Can they manage fine motor demands
- Can they return to school, work, equipment handling, and upper-extremity function that matters to them
How that shows up in sports rehab
For athletes, this split makes a lot of sense. A PT often rebuilds the physical engine. An OT often makes sure that engine can do the exact task you care about.
If you're trying to understand why this matters in training, it helps to think in terms of movement quality and transfer. This practical guide to functional strength is a useful primer because it connects strength work to real-world movement instead of treating exercise like a separate activity.
Shared goal, different lens. PT restores movement capacity. OT restores task performance and participation.
That difference isn't abstract. It changes what gets measured, what gets trained, and what “cleared to return” means for the athlete in front of you.
A Side by Side Comparison PT vs OT
The cleanest way to understand physical therapy vs occupational therapy is to put them side by side. In sports rehab, the overlap is real, but the lead focus is different.
Physical Therapy vs Occupational Therapy at a Glance
| Criterion | Physical Therapy (PT) | Occupational Therapy (OT) |
|---|---|---|
| Primary focus | Movement quality and body mechanics | Task performance and meaningful daily activity |
| Best known for | Restoring mobility, strength, balance, and range of motion | Restoring hand use, fine motor control, and functional independence |
| Movement emphasis | Gross motor performance | Fine motor performance and task execution |
| Common measures | Gait, balance, loading tolerance, joint motion, strength | Independence with tasks, hand function, visual-perceptual demands, work or school participation |
| Typical athlete goals | Run, jump, cut, lift, squat, land, throw, accelerate | Grip equipment, manage self-care, write, type, dress, handle tools, perform hand-based sport tasks |
| Common body regions | Lower extremity, spine, shoulder, whole-body movement | Hand, wrist, elbow, upper extremity task use, daily function |
| After surgery | Rebuild movement system and physical capacity | Rebuild how the athlete actually uses the arm or hand in life and sport |
| Main question asked | “Can your body do the movement?” | “Can you complete the task that matters?” |
A key distinction is that physical therapy is optimized around gross motor performance, while occupational therapy is optimized around fine motor performance and task execution, including hand function, visual-perceptual skills, and sensory processing, as explained by NAPA Center's breakdown of OT and PT.
Where athletes get confused
The confusion usually happens with upper-body injuries.
A shoulder problem can be a PT case if the issue is pain, range of motion, strength, or movement mechanics. The same shoulder problem can have an OT-heavy component if the athlete still can't dress normally, carry gear, control hand use during daily tasks, or return to fine motor demands.
The same is true for wrist and hand injuries. Athletes often assume any orthopedic injury belongs with PT. That's too simplistic. If the main barrier is hand function, dexterity, and task execution, OT may be the better fit.
The better question is not “Which profession handles this diagnosis?” It's “Which profession handles the limitation that matters most right now?”
There's also a practical workforce distinction. In the United States, there were about 238,000 physical therapists in 2021, and the median annual salary for physical therapists in 2022 was $97,720, while for occupational therapists the Bureau of Labor Statistics projected 18% employment growth from 2019 to 2029 and reported a median annual wage of $84,270 in May 2018, according to WebMD's summary citing BLS data. For patients, the useful takeaway is simple. PT has a larger current workforce and higher median pay, while OT has shown strong projected growth.
What Conditions Do PTs and OTs Treat
A sports clinic sees plenty of overlap. Still, some conditions clearly lean one direction first.
Conditions that often fit physical therapy first
PT typically leads when the main problem is restoring the physical system. That includes pain-limited movement, reduced strength, restricted range of motion, balance issues, and sport mechanics.
Common examples include:
- ACL recovery: Rebuilding knee motion, quad strength, landing mechanics, cutting, and return-to-sport testing.
- Ankle sprains: Restoring mobility, calf strength, balance, and change-of-direction tolerance.
- Running injuries: Addressing gait issues, loading tolerance, hip and calf strength, and training errors.
- Post-op knee or shoulder rehab: Rebuilding joint motion and progressive strength after surgery.
- Back and hip pain in athletes: Improving movement patterns, force transfer, trunk control, and sport tolerance.
- Dance overuse injuries: Correcting mobility deficits, loading strategy, turnout control, foot and ankle capacity, and technique-related stress.
Conditions that often fit occupational therapy first
OT becomes especially relevant when the limiting factor is how someone completes a meaningful activity. That includes self-care, school tasks, work tasks, and hand-intensive function.
Common examples include:
- Hand and finger injuries: Especially when grip, dexterity, object handling, and fine motor control are disrupted.
- Wrist injuries: When the athlete can move somewhat but still can't write, type, grip, tape, dress, or use equipment effectively.
- Elbow to hand conditions: Cases where upper-extremity task performance matters more than pure force production.
- Post-surgical upper-extremity function: When daily use and hand-based function lag behind basic motion.
A useful clinical distinction is this: PT aims to reduce impairment and restore the physical system, while OT measures whether the patient can perform meaningful activities, especially when the problem is how they complete tasks like dressing, eating, or work, as described by Center for Bone and Joint's comparison of physical therapy and occupational therapy.
Where both may belong
Some injuries need both lenses from the start.
- Shoulder injuries: PT may restore motion and cuff strength. OT may address dressing, reaching, gear handling, and upper-extremity task use.
- Complex wrist or forearm injuries: PT may address broader strength and loading. OT may lead hand function and precise task performance.
- Post-surgical athletes: One clinician may rebuild capacity. The other may bridge that capacity into daily use and sport-specific tasks.
If you're unsure, don't guess based on the body part alone. Ask what the actual bottleneck is. That usually tells you more than the injury name.
Real World Scenarios for Athletes
In real life, athletes don't present as neat categories. They show up with a goal, a deadline, and frustration.

Scenario one ACL recovery
A high school soccer player tears an ACL. The athlete needs knee extension, flexion, quad recovery, strength progression, balance, force absorption, sprint progression, and eventually cutting and return-to-sport testing.
That's a PT-led case.
In a sports-focused setting, that may include manual therapy, progressive strength work, hop and landing progressions, and objective return-to-sport testing. If the athlete is also struggling with school movement, dressing, or using crutches and braces early on, that can bring in function-based coaching, but the primary rehab engine is physical therapy.
An athlete with a post-op knee doesn't just need “exercise.” They need staged loading, movement quality, and sport-specific progression.
Scenario two hand and wrist injury
A dancer falls during rehearsal and lands hard on the hand. Pain settles somewhat, but now turns, floor transitions, costume fasteners, note-taking, and basic grip tasks are all frustrating.
Athletes and parents often choose incorrectly. They hear “orthopedic injury” and assume PT first. But for upper-extremity cases, the best provider is often determined by the functional bottleneck. The same shoulder or hand issue may be a PT problem if the barrier is motion or strength, but an OT problem if the barrier is dressing, gripping tools, or performing work tasks, as explained by RSFH's discussion of OT versus PT.
That means the right answer for a wrist or hand injury may be:
- PT first: if the major issue is motion loss, pain, or force production
- OT first: if the major issue is hand use, fine motor skill, grip, or task execution
- Both: if the athlete has clear deficits in each lane
For athletes trying to keep lifting while a shoulder issue calms down, exercise selection matters too. This guide to strength training without shoulder pain is a practical example of modifying training instead of stopping everything.
Scenario three the runner with a stubborn problem
A runner from Raynham or East Bridgewater isn't dealing with a hand problem at all. They can tie shoes, work, and manage daily life. But they can't tolerate mileage, hills, speed, or longer runs without pain returning.
That's squarely in the PT lane because the limiting factors are movement efficiency, tissue loading, and performance mechanics. In that situation, a detailed running gait analysis can be one of the most useful next steps because it connects symptoms to stride mechanics, cadence strategy, and force management.
A short visual can help if you're trying to picture how movement retraining fits into sports rehab.
The point across all three examples is simple. Diagnosis matters, but functional goal matters more when you're deciding who should lead rehab.
Making the Right Choice for Your Recovery
If you're stuck between physical therapy vs occupational therapy, don't start with the profession title. Start with the problem you need solved.
Ask what is actually stopping you
Use these questions before you book:
- Is the main issue pain and movement loss? If you can't bend, straighten, lift, squat, jump, run, or load normally, PT is often the better first stop.
- Is the main issue task performance? If you can move somewhat but still can't grip, write, dress, manage gear, or perform fine motor tasks well, OT may be the better first stop.
- Is this an upper-extremity problem? Shoulder, elbow, wrist, and hand cases are where the distinction matters most.
- Do you need sport-specific progression? If the goal is return to sprinting, cutting, jumping, dance, lifting, or running mechanics, PT usually leads that part.
- Do you need adaptation or task retraining? If the underlying issue is how to perform meaningful daily or sport-related tasks, OT may lead.
For patients dealing with more complex rehab needs, it can also help to understand how specialized services are layered into a plan. This overview of advanced physical and aquatic therapy is useful because it shows how rehab can be matched to the person, not forced into one format.
A simple decision rule
Try this:
If the biggest problem is can't move well, think PT. If the biggest problem is can't do the task well, think OT.
That rule isn't perfect, but it's useful. It also explains why some athletes need both. A baseball player recovering from shoulder surgery may first need PT to restore range and strength, then OT support for the finer task demands of upper-extremity function in everyday life and sport.
Whatever you choose, don't rely on internet self-sorting alone. A licensed rehabilitation professional can tell pretty quickly whether the main barrier is body capacity, task performance, or a mix of both.
Your Integrated Recovery Team at Physical Therapy U
The best sports rehab clinics don't work in silos. They coordinate.
Why integrated care works better
That matters most in post-surgical recovery and upper-extremity cases. One clinician may focus on restoring mobility, strength, loading tolerance, and movement mechanics. Another may focus on hand use, task performance, and getting the athlete back to normal life outside the clinic.
For active patients in Bridgewater, Buzzards Bay, Middleborough, and nearby South Shore Massachusetts communities, integrated rehab can make the transition back to sport much cleaner. It reduces the gap between “your joint moves better” and “you can use it where it matters.”
In a sports-focused setting, that may include:
- Return-to-sport progression: Sprinting, jumping, cutting, deceleration, and testing
- Sport-specific services: Running gait analysis, dance therapy, and movement retraining
- Targeted treatment tools: Dry needling, hands-on therapy, and structured strengthening
- Upper-extremity recovery: Hand-to-elbow care when dexterity and task use are limiting progress
If you want a better sense of how sports-focused rehab fits into a larger recovery plan, this page on sports medicine and rehab gives a useful view of that model.
The main takeaway is straightforward. Athletes do best when the rehab plan matches the demand of the sport and the functional task, not just the diagnosis on paper.
Frequently Asked Questions About PT and OT
Can I need both PT and OT
Yes. That's common with shoulder, elbow, wrist, and hand injuries, and with some post-surgical recoveries. One discipline may rebuild physical capacity while the other helps translate that capacity into daily function, school demands, work tasks, or hand-based sport skills.
Which one is better for a shoulder injury
It depends on what's limiting you. If your main issue is pain, weakness, range of motion, or inability to press, throw, or stabilize, PT usually leads. If your shoulder moves better but you still can't dress, manage gear, use your arm effectively through daily tasks, or handle fine motor demands, OT may be important.
Is OT only for older adults or non-athletes
No. That's one of the biggest misconceptions. OT can be highly relevant for athletes, especially in upper-extremity rehab, hand function, post-surgical recovery, and return to normal task performance outside practice.
Is telehealth enough for sports rehab
Sometimes, but not always. A 2024 review noted the need for more evidence on how PT and OT services should be delivered to underserved or remote populations, which tells us access questions are still being worked out. The same review also supports a practical conclusion clinicians already see every day: telehealth is expanding, but the right choice between remote and in-person care depends heavily on the condition and whether hands-on treatment is needed, as discussed in this 2024 review of PT and OT service delivery for underserved groups.
In practice, telehealth can work better for exercise review, education, home progression, and some movement follow-up. It's less ideal when the athlete needs hands-on assessment, post-op measurement, manual treatment, splinting, or close in-person progression.
Do I need an evaluation even if I think I know which one I need
Yes. Self-diagnosis usually misses the underlying bottleneck. Athletes often describe the pain site accurately but misread the cause of the limitation. A good evaluation looks at movement quality, task demands, sport goals, aggravating loads, and what has to happen before a safe return.
What if I'm a runner, dancer, or field athlete with a very specific goal
Then general rehab usually isn't enough. You want someone who can connect symptom reduction to sport-specific loading. That may mean gait analysis for runners, landing and jump mechanics for court and field athletes, or dance-specific movement assessment for dancers.
If you're trying to sort out physical therapy vs occupational therapy and want athlete-centered guidance from licensed rehab professionals, Physical Therapy U can help. With locations in Bridgewater, Buzzards Bay, and Middleborough, PTU works with athletes, runners, dancers, and post-surgical patients across Southeastern Massachusetts to build clear, goal-driven rehab plans that get you back to sport with confidence.
{kind=link}