You cut hard to your left, your eyes stay on the ball, and for a split second the field lags behind your head. Or you finish a turn in dance class and feel like the room keeps moving after you stop. Or you're a few weeks out from knee surgery, walking fine in a straight line, but you still feel oddly unsteady when people move around you.
That “off” feeling matters in sports physical therapy because high-level movement depends on more than strength. Your brain has to match what your eyes, inner ear, neck, and legs are telling it in real time. When that system gets disrupted after a head knock, whiplash, surgery, illness, or a stretch of reduced training, performance drops fast. You may not describe it as vertigo. Most athletes don't. They say they feel foggy, slow to react, weird in busy environments, or less confident changing direction.
For athletes in Bridgewater, Massachusetts and across the South Shore, this is also why recovery habits matter outside the clinic. If you're already dealing with dizziness, visual overload, or delayed recovery, it's worth understanding sleep's role in athletic success, because poor sleep can make symptoms harder to tolerate and training harder to dose.
Table of Contents
- That Off Feeling Dizziness and Your Athletic Performance
- Why Vestibular Health Is Your Secret Performance Weapon
- The Four Pillars of Vestibular Rehab Your Starter Kit
- How to Progress Your Vestibular Training Safely
- Sample Vestibular Programs for Specific Goals
- Red Flags When to See a Physical Therapist at PTU
- FAQ Your Vestibular Rehab Questions Answered
That Off Feeling Dizziness and Your Athletic Performance
You clear warmups, but something still feels off. The soccer ball gets harder to track once play speeds up. The run feels fine on a treadmill, then turns shaky when you scan traffic, curbs, and other runners outside. A dancer can own the basics in rehearsal and still lose confidence the moment multiple turns return.
The vestibular system helps explain that gap. It helps your brain sort head movement, body position, and visual input fast enough to keep you oriented during motion. When that system is irritated or poorly coordinated, athletes often describe it the same way. Late reactions, blurred focus with head turns, hesitation on cuts, and a weird sense that the body is a half step behind.
I see this a lot in sports rehab. The athlete is strong enough. The knee may test well. The neck may be improving. But once the task involves turning the head, finding a target, and changing direction under speed, symptoms show up again.
Vestibular rehabilitation exercises retrain that link between the eyes, head, and body. The usual tools are habituation, gaze stabilization, and balance work, but the application matters. A field athlete needs drills that hold up during scanning and reactive movement. A runner may need symptom-free head motion integrated into stride mechanics, often alongside a running gait analysis for outdoor movement demands. A dancer may need graded turn exposure, spotting retraining, and better tolerance to repeated changes in head position. A post-op patient may need vestibular work blended with lower-body rehab so stability returns under real-world load, not just in a quiet clinic corner.
You do not need spinning vertigo for vestibular rehab to matter. Many athletes just feel less sharp, less stable, and less willing to trust movement.
There is a trade-off here. Push too little and the system never adapts. Push too hard and symptoms spike enough to change mechanics, increase guarding, and drain confidence. Sleep also affects how well athletes tolerate that training load, which is one reason sleep's role in athletic success deserves attention during rehab.
Generic handouts miss that return-to-sport gap. Athletes, dancers, and post-op patients do better when vestibular drills match the speed, visual demand, and positional stress of the activity they are trying to get back to.
Why Vestibular Health Is Your Secret Performance Weapon
Fast sport demands a stable visual system. If your eyes can't stay locked on the target while your head moves, you're slower reading the play, slower cutting, and slower trusting what you see.

Your inner gyroscope affects more than balance
The vestibular system isn't just about not falling over. It helps keep vision clear during movement through the vestibulo-ocular reflex, often shortened to VOR. In plain language, that reflex helps your eyes stay on the target while your head is moving.
For an athlete, that means things like:
- Tracking under speed: Keeping your eyes on a ball, teammate, defender, or landing spot while your body changes direction.
- Recovering after contact: Regaining visual and postural control after a bump, stumble, or awkward step.
- Handling visual chaos: Staying composed when the environment gets busy, like a crowded gym, race start, or dance rehearsal.
- Trusting deceleration: Feeling stable enough to stop, pivot, and re-accelerate without that split-second hesitation.
For runners, vestibular issues often show up as drift, tension, or discomfort in busy settings. If your form changes once your head starts moving more freely, a sports-specific screen like running gait analysis can help connect the dots between visual stability, stride mechanics, and confidence.
Why athletes and post-op patients notice it differently
A midfielder may notice delayed reaction and a hard time scanning left to right. A dancer may notice trouble spotting during turns or feeling unsteady after fast direction changes. A patient after ACL surgery may notice that single-leg tasks feel mechanically possible but neurologically shaky.
That last group gets overlooked. After surgery, people often focus on swelling, range of motion, quad strength, and hop testing. Those matter. But if an athlete still feels disoriented in motion, they won't fully trust return-to-sport demands.
Performance takeaway: A stronger leg doesn't automatically create a stable athlete. The brain still has to process motion cleanly.
This is why vestibular health becomes a performance tool, not just a symptom-management tool. When it's working well, movement feels crisp. When it isn't, athletes compensate with stiffness, caution, and slower decisions.
The Four Pillars of Vestibular Rehab Your Starter Kit
A runner who can squat heavy but gets disoriented during head turns does not need more random balance drills. A dancer who feels off after spotting practice does not need a generic handout. Vestibular rehab works best when the drills match the movement demands that trigger symptoms, and when the program builds from basic visual control to sport-speed balance.
A widely used clinical review describes a starter framework built around gaze-stability work plus balance and gait training, with frequent short bouts across the day rather than one long session for vestibular rehabilitation. In practice, I also organize athlete programs around a fourth bucket: habituation for movements that consistently provoke symptoms. For post-op patients, that same structure helps bridge the gap between “the joint is strong enough” and “the body trusts motion again.”
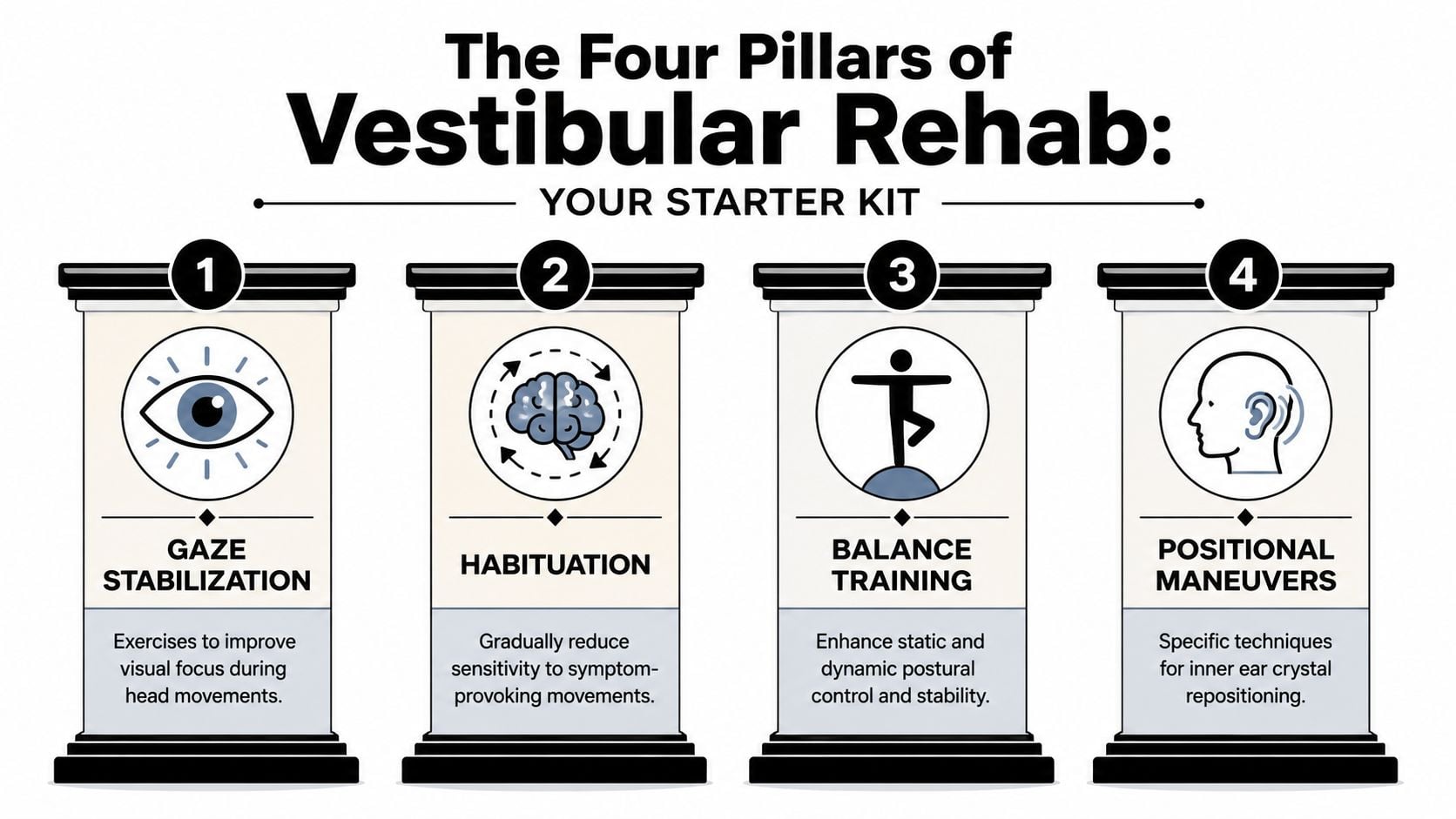
Gaze stabilization
Gaze stabilization trains the vestibulo-ocular reflex, or VOR. That reflex keeps your vision clear when your head moves. If it is underperforming, the room seems to lag, targets blur, and quick scanning gets uncomfortable.
For many athletes, a primary starting exercise is maintaining a clear target while the head moves.
A common starter drill is VOR x1 viewing.
- Set-up: Sit or stand facing a single target like a sticky note or letter on the wall.
- Action: Keep your eyes locked on the target while you turn your head side to side.
- Form rule: The target should stay readable. If it blurs badly or symptoms climb too high, reduce speed or range.
- Starter progression: Start with short bouts that create mild to moderate symptoms, then build duration as tolerance improves using the same reviewed protocol noted earlier.
Then add the vertical version.
- Vertical VOR x1: Keep your eyes fixed on the target while nodding up and down.
- Sport carryover: Useful for runners scanning terrain, basketball players changing eye level quickly, and dancers moving from floor work to upright transitions.
For athletes, this work should connect to the rest of training. It fits well alongside a strength and conditioning program for athletes, especially during return-to-play phases when the goal is clear vision under speed, fatigue, and direction changes.
Here's a visual overview before you try the basics at home.
Habituation
Habituation is exposure training for movements that predictably bring on dizziness. The goal is not to avoid those movements. The goal is to reduce the alarm response to them.
A basic starting point might include:
- Sit to side-lying transitions: Move from sitting to lying on one side, return to sitting, then repeat to the other side.
- Head turn exposure: Turn your head toward the side that usually bothers you, pause, and return to center.
- Dose rule: Begin with a small, repeatable number of reps. Then increase gradually as long as symptoms settle in a reasonable time.
This pillar matters for athletes because their triggers are rarely generic. A soccer player may react to quick left-right scanning. A dancer may react to turns and spotting. A post-op athlete may react when the visual system gets stressed during split-stance or single-leg tasks, even though strength testing looks good.
Repetition drives adaptation. Infrequent, inconsistent exposure rarely changes much.
Balance training
Balance training restores postural control when visual input, head motion, or surface demands increase. Early drills can look basic, but the target is not standing still forever. The target is clean control that holds up when the environment gets busier.
Useful beginner drills include:
- Feet together standing: Stand tall with a narrow base. Keep your ribs stacked over your pelvis and breathe normally.
- Tandem stance: Place one foot directly in front of the other. Hold while keeping your eyes steady.
- Single-leg balance with a visual target: Stand on one leg while looking at a fixed point.
- Head turns in stance: Once basic standing is controlled, add slow side-to-side head motion without losing posture.
Then the progression needs to look more athletic. Add split stance, step-and-hold work, landing control, ball tracking, or reaching tasks. For a dancer, that may mean balance with spotting demands. For a field athlete, it may mean visual tracking during cuts. For a post-op patient, it may mean rebuilding single-leg confidence before return-to-sport testing.
Gait retraining
Walking exposes vestibular problems fast because it combines forward motion, head movement, visual flow, and postural control all at once.
Start with drills that stay controlled:
- Walk straight while turning your head left and right: Keep the path straight and your eyes level.
- Walk with up and down head motion: Nod while continuing forward.
- Change surfaces carefully: Progress from stable flooring to more challenging environments once basic control is reliable.
For athletes, gait work is the bridge to real movement. Progress from walking to jogging, then to reactive motion that matches the sport.
- Runner progression: Walk, then jog while scanning side to side.
- Field sport progression: Add target calls, reactive turns, or cone changes.
- Dance progression: Add spotting, directional changes, and controlled turn entry.
The biggest mistake across all four pillars is dosing poorly. Too little challenge does not drive adaptation. Too much challenge creates sloppy movement, visual loss, and symptom flare-ups that carry into the rest of the day. The best programs sit in the middle and progress toward the exact demands your sport, performance setting, or recovery phase requires.
How to Progress Your Vestibular Training Safely
You finish a set of head turns, stand up to jog, and the room feels a half-step behind you. That does not automatically mean the drill was wrong. It usually means the dose needs work.
Vestibular rehab improves through repeated, tolerable exposure. For an athlete, dancer, or post-op patient, the goal is not to chase symptoms or avoid them completely. The goal is to create enough challenge that the brain adapts, while movement quality stays clean and recovery stays predictable.
Find the right symptom zone
A good session creates a small, controlled rise in symptoms that settles soon after the set. I want athletes to feel challenged, not rattled. If vision blurs, posture locks up, or nausea keeps building, the drill has crossed the line from training to overload.
Use three checks:
- Mild symptom increase: You notice dizziness, visual strain, or a sense of disorientation, but you can still stay on task.
- Short recovery: Symptoms ease with brief rest and do not hijack the next part of the session.
- Repeatable quality: You can do the next rep or set with the same control.
Watch for the wrong response:
- Big symptom spike: You feel overwhelmed, lose the target, or need to stop abruptly.
- Long recovery: Symptoms keep rolling long after the set ends.
- Technique breakdown: You hold your breath, stiffen through the trunk, or start moving randomly instead of following the drill.
Practical rule: If the drill is so hard that you cannot train the intended skill, change the dose.
That trade-off matters in sport. A soccer player has to keep visual focus while cutting. A dancer has to control spotting without drifting off axis. A post-op patient has to rebuild head and body movement together, not just survive a symptom-provoking exercise.
Progress one variable at a time
Change one thing, then reassess. That is how you know whether the improvement came from speed, stance, surface, or visual complexity.
Progress a drill by adjusting one of these:
- Head speed: Turn or nod faster only if the target stays clear.
- Body position: Move from sitting to standing, then split stance, then single-leg.
- Visual environment: Start with a plain wall, then add a busier background.
- Support surface: Use foam or a pillow only after firm ground is easy.
- Task complexity: Add catching, footwork, ball tracking, or reaction cues.
Regress a drill if control falls apart:
- Sit instead of stand
- Slow the head motion
- Use a smaller range
- Shorten the work interval
- Return to a simpler room setup
For runners, this often means earning clear vision during head motion before adding mileage or pace. If return to running is part of the plan, these physical therapy exercises for runners pair well with vestibular progressions because they rebuild impact tolerance and single-leg control at the same time.
Match the progression to the sport or recovery stage
Generic online progressions miss this point. The finish line is different for each person.
A basketball guard may need gaze stability while backpedaling and reading movement in the periphery. A dancer may need repeated turn entry, spotting, and landing control. A gymnast may need head movement tolerance during inversion and fast direction changes, which is why some coaches also review gymnastics programming tips alongside rehab planning. A post-op patient may need a slower build, with more attention to fatigue, neck stiffness, and confidence during single-leg tasks.
Progression should reflect that reality. Start with the cleanest version of the skill. Then add speed, visual demand, and decision-making in the same order the athlete will need them back in practice or performance.
Done well, vestibular progression looks boring at first and very specific later. That is usually a good sign.
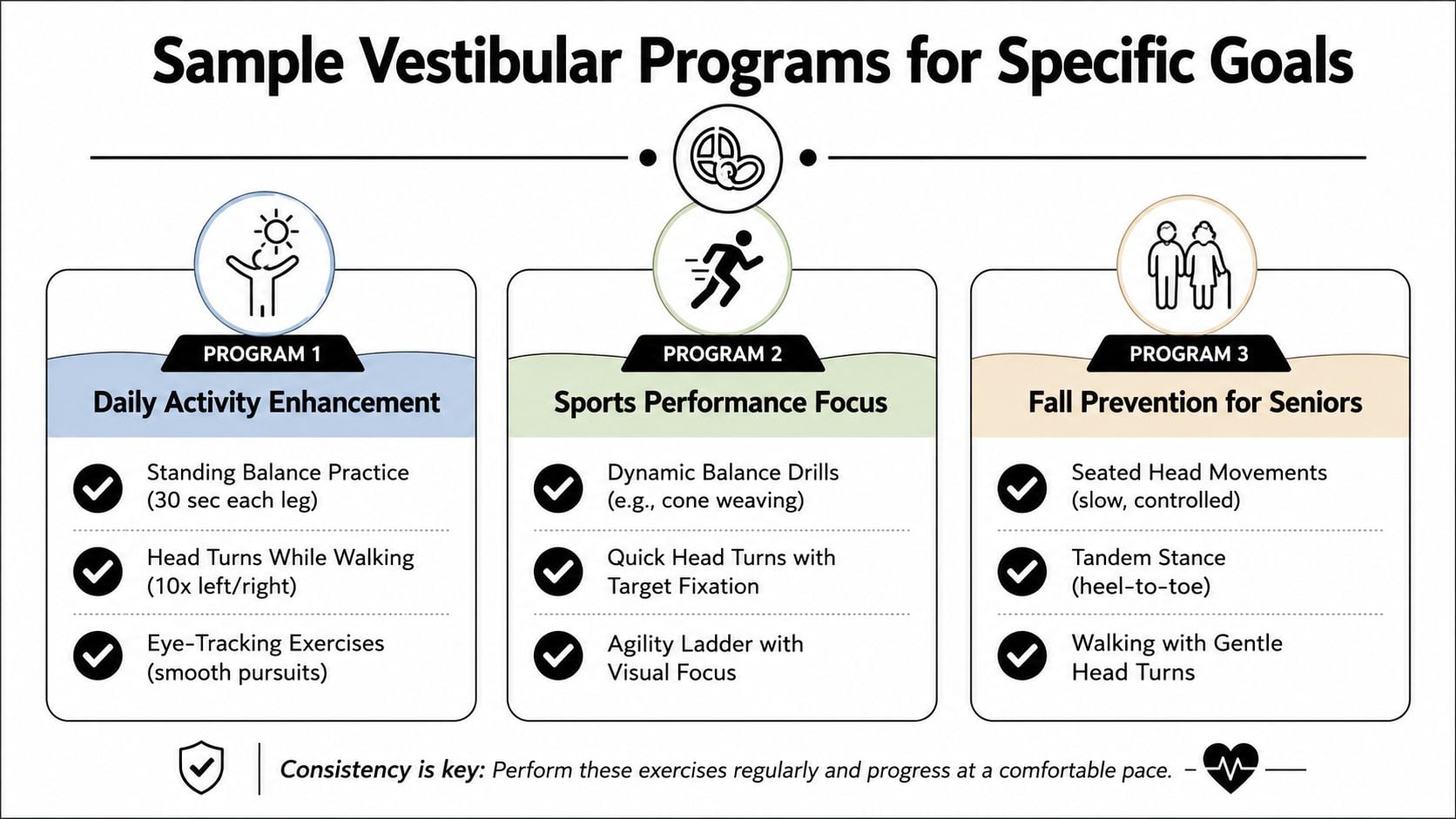
Sample Vestibular Programs for Specific Goals
A soccer player cuts to the left, lifts her eyes to track the ball, and the field smears for a second. A dancer finishes a turn and needs an extra beat to find center. A patient after knee surgery walks through a busy hallway and feels unsteady even though the knee itself seems solid. Those are all vestibular complaints, but they do not call for the same drill list.
At PTU, the program starts with the task that breaks down. Then we choose exercises that match the trigger, the sport, and the recovery stage. Generic handouts miss that level of specificity.
Post-concussion field athlete
A field athlete after concussion often says, "I can jog, but I lose the play when I turn my head." That points to a gap between basic movement tolerance and sport-speed visual processing.
A useful starter plan may include:
- VOR x1 at a letter target: Keep the eyes clear while the head moves side to side, then up and down.
- Walking with head turns: Start in a quiet hallway, then build toward busier visual environments.
- Scan and react drills: Shuffle or jog to cones while finding numbers, colors, or coach signals.
- Sub-symptom aerobic work: Bike, treadmill, or light field movement that raises effort without causing a prolonged flare.
The trade-off is simple. If you push visual complexity too early, mechanics usually get sloppy and symptoms linger. If you stay too basic for too long, the athlete feels fine in the clinic and still struggles in practice.
Dancer with dizziness during turns
Dancers rarely need "better balance" in a generic sense. They need clear spotting, reliable head control, and the ability to enter and exit rotation without losing timing.
A program for that goal may include:
- Spotting on a fixed target: Eyes lock first, then the head and trunk follow.
- Turn-entry repetition: Practice the exact prep that brings on symptoms before returning to full combinations.
- Single-leg balance with port de bras or head motion: Build control in the positions that matter on stage.
- Graduated rotational exposure: Quarter turns, half turns, single turns, then linked sequences.
For dancers and gymnasts, I also look at how the skill is built. Good rehab and good coaching should agree on progression. Resources like these gymnastics programming tips can help frame how to break a complex movement into manageable pieces.
Post-op knee patient rebuilding confidence
After ACL reconstruction or another knee procedure, some athletes tell me the leg feels strong enough but the body still feels off in motion. They are often describing a mix of deconditioning, visual-motion sensitivity, and reduced confidence during head movement.
A practical early program may include:
- Quiet standing with visual fixation: Find steady posture before adding motion.
- Step-and-hold with head turns: Keep the knee organized while the vestibular system works harder.
- Walking drills with horizontal and vertical gaze shifts: Restore smooth movement through space.
- Marching, skipping, and low-level change-of-direction work: Prepare for impact and faster locomotion.
Once visual clarity during movement improves, the lower body work needs to catch up. For that next phase, these physical therapy exercises for runners fit well with vestibular progressions because they build load tolerance, single-leg control, and return-to-run capacity.
Sample programs help. Good results come from matching the drill to the functional demand, whether that is reading the field, finishing a pirouette, or trusting a post-op leg in motion.
Red Flags When to See a Physical Therapist at PTU
Home vestibular rehabilitation exercises can be productive. They can also be the wrong first move. The most common mistake is assuming every kind of dizziness should be treated with the same head-turn drills.
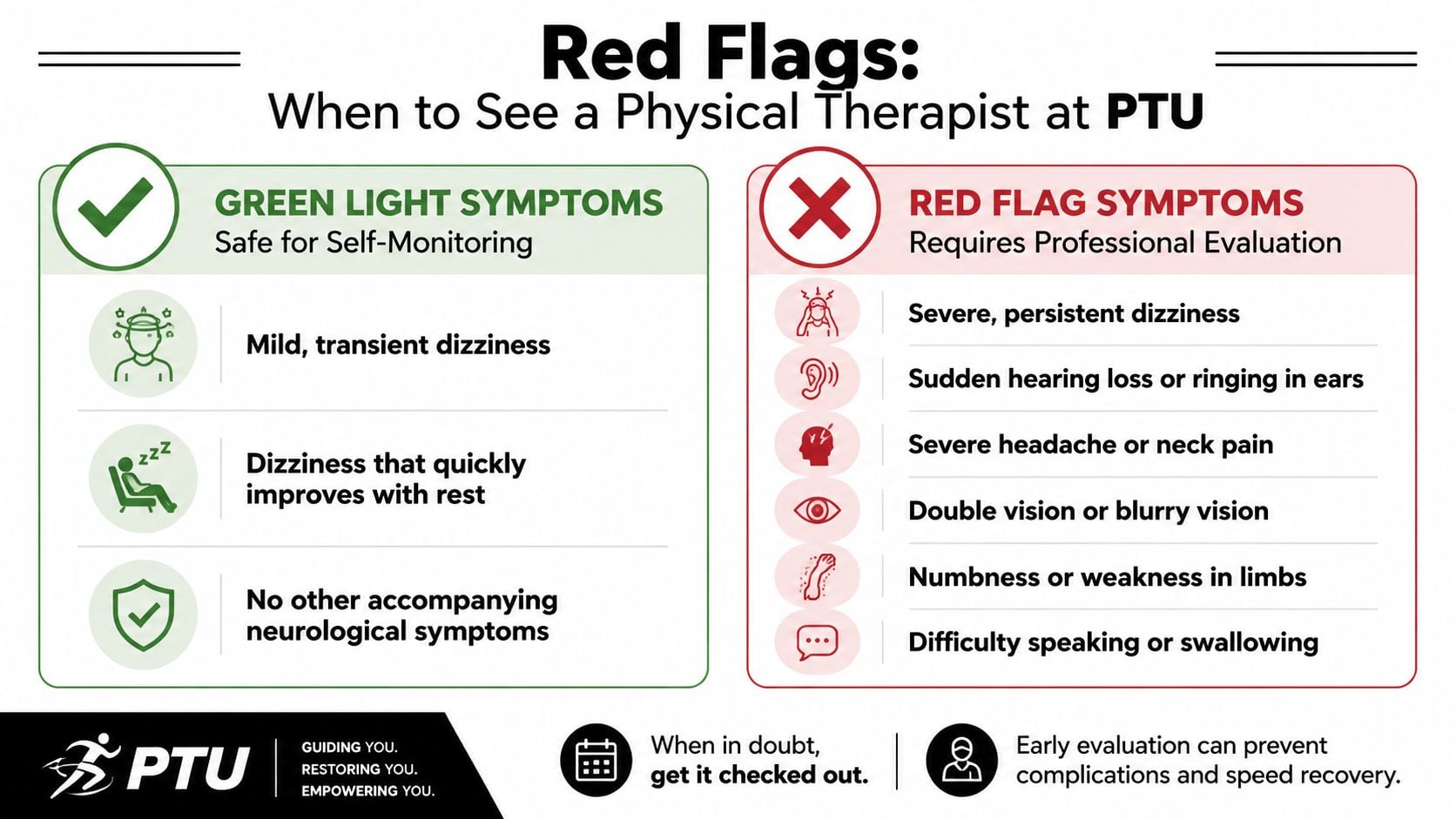
Green light versus stop and get checked
Use common sense here. Mild, brief symptom provocation during a correctly chosen exercise can be normal. Worsening, confusing, or severe symptoms are different.
Green light signs
- Mild temporary dizziness: Symptoms rise a little during the drill, then settle.
- Clear trigger pattern: You know which movement brings it on and the response is consistent.
- Stable overall picture: No major new symptoms outside the exercise session.
Red flag signs
- Severe or escalating dizziness: Especially if it's getting worse rather than gradually improving.
- Sudden hearing changes: New hearing loss or ringing should not be ignored.
- Severe headache or neck pain: Especially after trauma or if it feels unusual for you.
- Double vision, weakness, numbness, trouble speaking, or trouble swallowing: These require prompt medical attention.
When exercises are the wrong first step
It's also important to separate VRT from canalith repositioning maneuvers. Authoritative guidance from the Canada balance center's vestibular rehabilitation overview explains that maneuvers like the Epley are used for repositioning ear crystals in BPPV, while vestibular rehab focuses on adaptation to vestibular deficits. If dizziness worsens instead of trending in the right direction, reassessment makes more sense than adding more reps.
That matters for athletes with positional vertigo, post-concussion symptoms, mixed neck and vestibular issues, or post-surgical patients whose movement confidence hasn't returned. Sometimes the answer is gaze stabilization. Sometimes it's a repositioning maneuver. Sometimes it's a cervical assessment. Sometimes it's all of the above, in the right order.
FAQ Your Vestibular Rehab Questions Answered
How long does vestibular rehab take
Timelines vary. According to the Cleveland Clinic's vestibular rehabilitation guidance, some patients improve in 1 to 2 sessions, a typical course is 6 to 8 weekly sessions, and others may need treatment for several months. Home exercises are often prescribed 2 to 3 times per day.
For athletes, the symptom timeline and the performance timeline aren't always the same. You might feel better before you're ready for full game speed or repeated turns.
Is it normal to feel a little worse at first
Sometimes, yes. Vestibular rehab often works by exposing you to movements that bring on a mild and temporary symptom response. That's different from a major flare that knocks you out for the rest of the day.
If symptoms become excessive, the answer usually isn't to quit everything forever. It often means the exercise, speed, position, or volume needs to be adjusted.
Mild challenge is useful. Symptom chaos is not.
What if I also have neck pain
That's common, especially after concussion, whiplash, or sports contact. Neck dysfunction can contribute to dizziness, motion sensitivity, and a general “off” feeling. If turning your head is painful or your symptoms feel tied to neck position, you need an in-person assessment rather than a generic handout.
This is one reason athletes do better with a sports physical therapist who can separate vestibular issues from cervical issues, then build both back together.
What is the difference between dizziness and vertigo
People use the words interchangeably, but they're not identical. Dizziness is a broad term that can include lightheadedness, fogginess, imbalance, or disorientation. Vertigo more specifically refers to a spinning or motion sensation.
That distinction helps guide treatment. Positional spinning may point toward crystal-related vertigo. Visual-motion sensitivity during sport may point more toward a vestibular adaptation problem.
If you're an athlete, runner, dancer, or post-op patient in Bridgewater, Buzzards Bay, Middleborough, or nearby South Shore Massachusetts towns like Plymouth, Taunton, East Bridgewater, West Bridgewater, and Raynham, a personalized exam matters. Physical Therapy U provides athlete-centered care reviewed by licensed DPTs, with sport-specific rehab, return-to-sport testing, running gait analysis, dance therapy, and hands-on treatment options including dry needling when appropriate. Book an evaluation to get a plan that matches your symptoms, your sport, and your next goal.
{kind=link}