Your elbow doesn't always hurt where the primary issue lies. If you're a pitcher, lifter, runner who works at a desk, dancer doing repeated floorwork, or a grappler spending a lot of time with the elbow bent, you may notice an ache on the inside of the elbow, tingling into the pinky and ring finger, or a hand that suddenly feels less reliable. Those are classic clues that the ulnar nerve is getting irritated.
At PTU, we look at this through a sports physical therapy lens first. For athletes in Bridgewater, Massachusetts and across the South Shore Massachusetts area, the question usually isn't just “What is this?” It's “Can I keep training?” and “How do I get back without making it worse?” That's the right focus.
Table of Contents
- What Is Cubital Tunnel Syndrome?
- Why Your Funny Bone Nerve Is Causing Elbow Pain
- Recognizing the Signs of Cubital Tunnel Syndrome
- How Physical Therapy Can Help You Avoid Surgery
- When Is Surgery the Right Call for Cubital Tunnel?
- Preventing Cubital Tunnel Syndrome in Your Sport
- Frequently Asked Questions About Elbow Pain
- Your Next Steps for Elbow Pain Relief on the South Shore
What Is Cubital Tunnel Syndrome?
Cubital tunnel syndrome is a compression problem involving the ulnar nerve as it passes along the inside of the elbow. It's one of the most common nerve compression issues in the upper extremity. In active people, it often shows up as cubital tunnel syndrome elbow pain plus numbness or tingling into the ring and little fingers.
The pattern matters. Elbow pain alone can come from tendon overload, joint irritation, or even the neck. But when the inside of the elbow hurts and your pinky-side fingers feel strange, a nerve problem moves much higher on the list.
This isn't a rare issue. A population-based survey found that between 1.8% and 5.9% of healthy adults reported symptoms consistent with cubital tunnel syndrome in a sample of 1,001 adults (population data on cubital tunnel prevalence). That same review also describes it as the second most common compression neuropathy of the upper extremity.
The biggest mistake athletes make is treating this like ordinary soreness for too long. Nerve symptoms usually need a different plan than muscle soreness.
For athletes, dancers, and active adults, the practical issue is simple. Nerves don't like repeated compression, repeated tension, or long stretches in a provoked position. If your training or daily setup keeps feeding those stresses, symptoms tend to hang around.
The good news is that many cases respond well when you catch the pattern early, reduce the right irritants, and rebuild movement around the elbow, shoulder, wrist, and neck with a licensed physical therapist.
Why Your Funny Bone Nerve Is Causing Elbow Pain
The “funny bone” feeling is a familiar sensation. You bump the inside of your elbow and get a sharp zing down the forearm into the hand. That sensation happens because you hit the ulnar nerve.
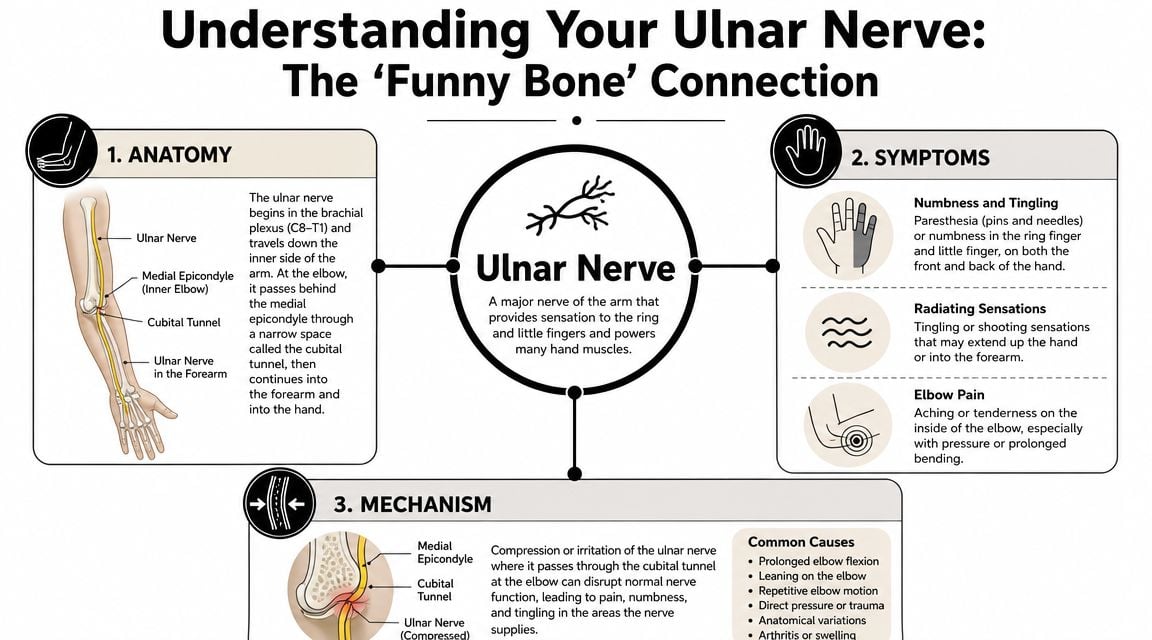
The nerve gets irritated at a tight corner
At the elbow, the ulnar nerve passes through a narrow region behind the medial epicondyle, the bony area on the inside of the elbow. Cubital tunnel syndrome is a compressive neuropathy of the ulnar nerve at the medial elbow, and elbow flexion plus direct pressure can significantly increase mechanical stress on the nerve (clinical overview of cubital tunnel mechanics).
A simple way to picture it is a garden hose at a corner. If the hose gets bent hard or pinned against an edge, flow becomes less smooth. A nerve isn't a hose, but the analogy helps. Repeated bending and pressure reduce how comfortably that tissue moves and tolerates load.
Why athletes feel it during normal training
This is why symptoms are often position-dependent. You may be fine with the elbow relatively straight, then symptoms ramp up when the elbow stays bent for a while or when you lean on it.
Common athletic triggers include:
- Throwing volume: Repeated elbow motion can irritate an already sensitive nerve.
- Lifting posture: Deep elbow flexion, aggressive pulling volume, or resting between sets with elbows bent and compressed can provoke symptoms.
- Dance positions: Floorwork, arm support positions, and sustained elbow flexion can load the area in ways dancers don't always recognize right away.
- Grip-heavy sports: If hand muscles start working around a sensitized ulnar nerve, symptoms can spread into the forearm and hand.
Practical rule: If your symptoms are much worse when your elbow stays bent, the nerve is telling you that position matters.
That's also why random stretching or “loosening everything up” doesn't always help. If the problem is mechanical stress on the nerve, the fix has to address the positions, loads, and movement habits causing that stress.
Recognizing the Signs of Cubital Tunnel Syndrome
Athletes often wait too long because the early signs seem inconsistent. One practice feels fine. The next day your elbow aches, your pinky tingles, and your grip feels off.

What athletes usually notice first
The hallmark symptoms are fairly specific:
- Tingling in the ring and little fingers
- Numbness that comes on with elbow bending
- Aching along the inside of the elbow
- Hand weakness, especially with grip or fine finger control
- Symptoms at night, especially if you sleep with the elbow curled up
That symptom pattern helps separate this from other problems. Tennis elbow usually hurts more on the outside of the elbow and is less likely to create finger numbness. A neck issue can refer symptoms into the arm, but it often has a different distribution and may change more with neck movement than elbow position.
What an evaluation looks like
In a sports PT exam, we don't just ask where it hurts. We look at what loads the tissue, what position brings symptoms on, and what your sport demands.
A useful cubital tunnel evaluation usually includes:
- Symptom mapping: Where exactly do you feel tingling, pain, or weakness?
- Elbow flexion testing: Does holding the elbow bent reproduce symptoms?
- Tinel's sign at the elbow: Tapping over the nerve to see if it creates the familiar tingling pattern
- Strength screening: Grip, finger control, and intrinsic hand function
- Movement assessment: Throwing mechanics, lifting form, dance demands, or work posture
- Regional screen: Neck, shoulder blade control, wrist, and forearm mobility
Some athletes come in convinced they need to stop everything. Others try to power through until hand weakness shows up. Neither extreme is ideal.
A better approach is to get a clear diagnosis early. Because this condition is common, it's worth taking seriously. In that same population review cited earlier, cubital tunnel syndrome was described as a common source of elbow and hand symptoms in active adults. That fits what we see clinically. It's easy to miss if you only think “elbow pain” and ignore the nerve pattern.
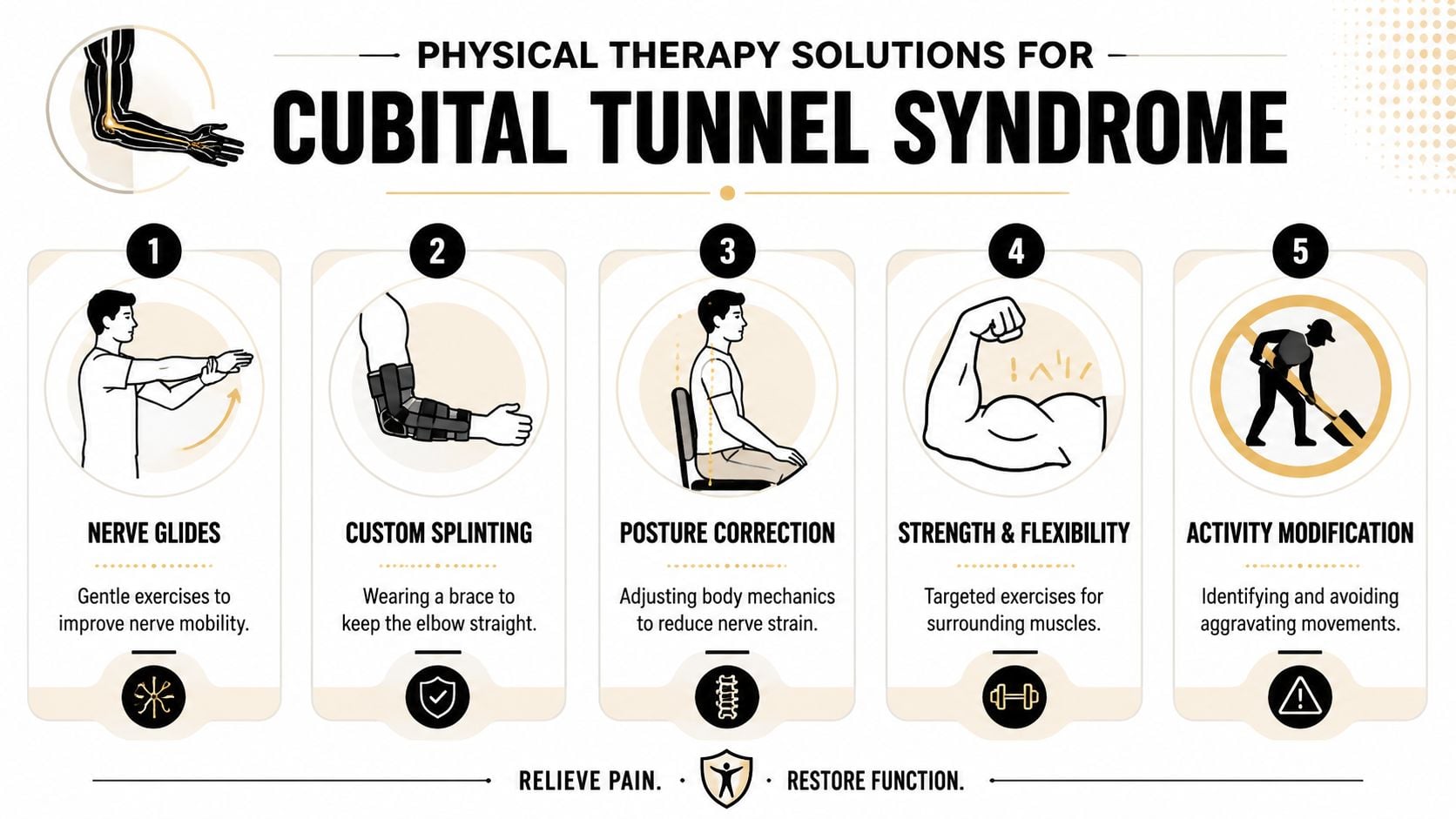
How Physical Therapy Can Help You Avoid Surgery
Early treatment works best when it is specific. The goal isn't to throw random exercises at the elbow. The goal is to reduce the mechanical stress bothering the nerve, calm symptoms down, then rebuild tolerance for sport.
What tends to work
For most athletes, the first win is reducing the positions that keep flaring the nerve. That usually means changing training, sleep position, desk setup, and recovery habits for a period of time.
A practical PT plan often includes:
- Activity modification: Temporarily reducing repeated elbow flexion, leaning on the elbow, or high-volume gripping that reproduces symptoms.
- Night positioning or splinting: Keeping the elbow from spending hours tightly bent during sleep.
- Nerve mobility drills: Gentle ulnar nerve glides when they calm symptoms rather than provoke them.
- Strength work upstream and downstream: Scapular control, rotator cuff strength, forearm capacity, and hand function when tolerated.
- Technique review: Throwing mechanics, lifting setup, dance-specific arm loading, or work ergonomics.
- Manual therapy: Addressing surrounding soft tissue stiffness that may add to local irritation.
- Progressive return to sport: Building exposure back up instead of guessing.
At PTU, that can also include services such as dry needling, laser therapy, myofascial work, sport-specific training, dance therapy, running gait analysis when arm carriage matters, and formal return-to-sport testing when an athlete needs objective progression. For athletes who need broader rehab support, advanced physical and aquatic therapy options can also be part of the continuum depending on the presentation.
This video gives a helpful visual overview of conservative management ideas:
What usually doesn't work
A few things commonly stall progress:
- Training straight through numbness: Pain tolerance doesn't equal nerve tolerance.
- Aggressive stretching into symptoms: If tingling gets sharper or lingers after the drill, that's not productive.
- Only treating the elbow: Shoulder control, thoracic position, wrist demand, and sport mechanics often matter.
- Stopping all movement for too long: Complete shutdown can create deconditioning and make return harder.
- Using a brace but changing nothing else: Bracing helps some athletes, but it won't fix a throwing pattern, a poor lifting setup, or nightly elbow compression on its own.
If symptoms increase during a drill and stay worse after, the dose is wrong. Good rehab should calm the system, not keep poking it.
A sample progression might look like this:
| Phase | Main focus | Common decisions |
|---|---|---|
| Early irritation | Calm symptoms | Reduce aggravating positions, improve sleep posture |
| Subacute phase | Restore motion tolerance | Add gentle nerve mobility and low-load strength |
| Reloading phase | Rebuild sport capacity | Reintroduce gripping, upper-body loading, or skill work gradually |
| Return phase | Test performance | Progress toward full training with symptom monitoring |
The trade-off is straightforward. If you return too early, the nerve usually reminds you. If you unload forever, you lose strength and confidence. Good sports PT lives in the middle.
When Is Surgery the Right Call for Cubital Tunnel?
Most athletes want to avoid surgery, and that's a reasonable goal. But surgery is sometimes the right move, especially when the nerve is staying compressed long enough that strength begins to decline.
Signs it's time to get a surgical opinion
In a large U.S. insurance-claims analysis, researchers identified 53,401 new cases of cubital tunnel syndrome from 2006 to 2012, with an adjusted incidence of 30.0 cases per 100,000 person-years. In that cohort, 41.3% of patients eventually underwent surgery, and the proportion rose with age from 34.4% in people aged 18 to 30 to 48.8% in those aged 60 to 65 (large epidemiologic study of cubital tunnel treatment rates).
That doesn't mean surgery is inevitable. It does mean this condition can become serious enough that conservative care isn't enough for everyone.
Authoritative orthopedic guidance frames surgery around persistent symptoms, muscle weakness, or nerve damage, with the goal of preventing motor denervation and decompressing the nerve before weakness becomes irreversible. Procedures may include release, medial epicondylectomy, or anterior transposition depending on the mechanics of the nerve at the elbow (AAOS guidance on ulnar nerve entrapment and surgery).
What rehab looks like after surgery
If surgery is needed, rehab still matters a lot. Athletes usually need a staged plan to restore elbow motion, manage scar sensitivity, rebuild grip and upper-extremity strength, and return to skill work without re-irritating the nerve.
For throwers, lifters, dancers, and court-sport athletes, post-op rehab also has to answer sport-specific questions:
- When can the elbow tolerate repetitive flexion again?
- When can gripping volume go up?
- Does the athlete still compensate at the shoulder or wrist?
- Are they ready for return to play, or just eager?
That's where return-to-sport testing helps. Clearance shouldn't be based only on time. It should match what your sport asks your arm and hand to do.
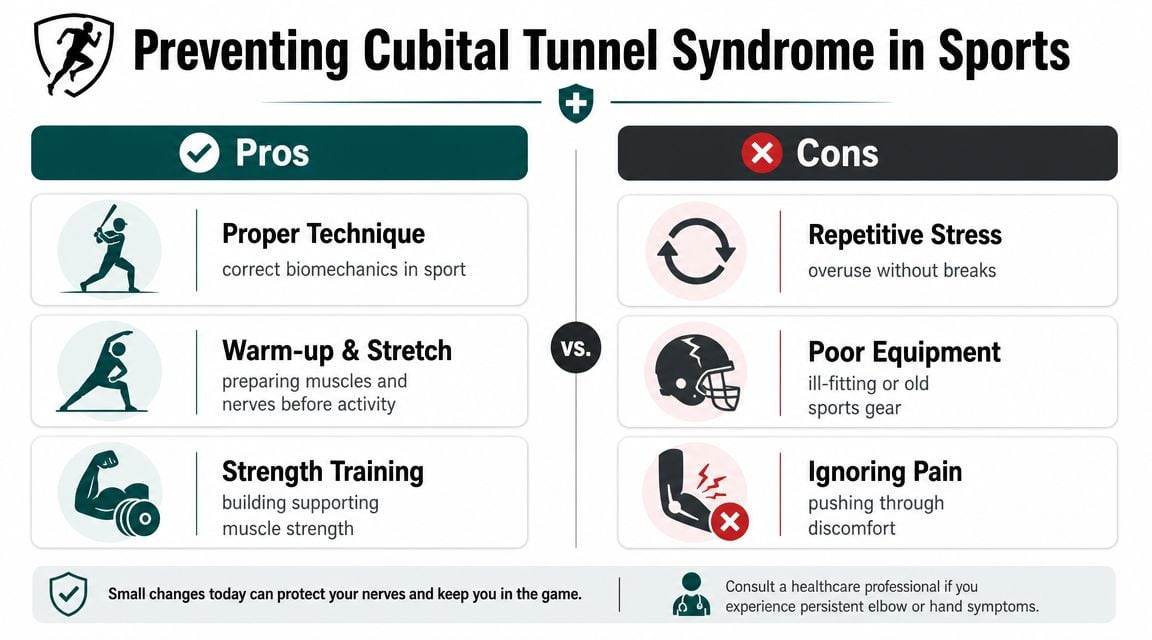
Preventing Cubital Tunnel Syndrome in Your Sport
Prevention isn't just about avoiding pain. The bigger goal is protecting the nerve before weakness develops. The reason that matters is simple. Orthopedic guidance stresses that prevention and conservative care aim to avoid motor denervation, and surgery is often considered once weakness appears.
Sport-specific habits that lower nerve stress
Different sports create different problems.
For throwers, the biggest issue is often accumulated irritation. Long throwing sessions, long car rides with the elbow bent afterward, and sleeping curled up can stack stress on the same tissue.
For lifters, the trap is usually exercise selection and setup. Deep elbow flexion under repeated load, sloppy upper-body positioning, and grip-heavy volume on top of tired tissue can keep symptoms active.
For dancers, floorwork, arm-supported transitions, and repeated end-range positions deserve attention. Dance therapy can help sort out what's coming from technique, rehearsal load, or recovery habits rather than blaming the whole problem on flexibility.
Grapplers and combat sport athletes deal with another layer. Repetitive gripping, clinch positions, and bent-elbow pressure add up fast. If you train jiu-jitsu, these Sydney BJJ training insights are a useful reminder that strength and conditioning should support tissue tolerance, not just mat conditioning.
A simple prevention checklist
Use this as a quick screen:
- Do keep the elbow straighter during sleep if nighttime numbness is a pattern.
- Don't lean on hard surfaces with the inside of the elbow compressed.
- Do build shoulder and upper-back strength so the elbow isn't doing more than it should.
- Don't ignore finger tingling just because the pain feels “minor.”
- Do adjust training volume early when symptoms first appear.
- Don't keep repeating the exact movement that causes numbness and hope it fades on its own.
- Do use sport-specific strength work to improve load tolerance. PTU's strength and conditioning program for athletes is one example of how that can fit alongside rehab.
- Don't forget daily posture and work setup if you spend hours typing, driving, studying, or gaming between practices.
Small changes in elbow position, sleep posture, and training volume can make a big difference because this is often a position-driven problem.
Frequently Asked Questions About Elbow Pain
Is cubital tunnel syndrome the same thing as tennis elbow
No. Tennis elbow usually affects the outside of the elbow and is more of a tendon overload problem. Cubital tunnel syndrome involves the ulnar nerve on the inside of the elbow and more often includes tingling or numbness into the ring and little fingers.
Can I keep working out if I have cubital tunnel syndrome elbow pain
Usually yes, but not exactly the same way you are now. The right move is to keep training around the problem instead of feeding it. That may mean lowering gripping volume, changing pressing or pulling variations, reducing prolonged elbow flexion, or temporarily modifying throwing or dance workload. If symptoms spread, linger, or your hand feels weaker, get evaluated.
Why do my symptoms get worse at night
Many people sleep with the elbow bent tightly. That position can increase stress on the ulnar nerve, so you wake up with numb fingers or an aching elbow. Sometimes a simple change in sleep positioning helps a lot. Sometimes you need a more structured rehab plan because daytime training and work habits are also driving the irritation.
Does dry needling help cubital tunnel symptoms
It can help some athletes, but not because it “fixes the nerve” by itself. Dry needling may reduce surrounding muscle tension and help with local pain in the forearm, triceps, or shoulder region when those tissues are contributing to the problem. It works best as part of a larger plan that includes load management, nerve mobility, strength, and movement changes.
How long does physical therapy take
It depends on how irritated the nerve is, whether you already have weakness, and whether your sport keeps reloading the same position. Mild cases may settle relatively quickly once you stop provoking them. More stubborn cases take longer because the plan has to calm the nerve and rebuild tolerance. The timeline should come from an in-person evaluation, not from a generic internet estimate.
Do I need imaging or nerve testing right away
Not always. Many cases can be identified clinically from the symptom pattern and exam. But if symptoms are progressing, weakness is appearing, or the diagnosis isn't clear, a physician may recommend further testing. A licensed PT can help determine when a referral makes sense.
Your Next Steps for Elbow Pain Relief on the South Shore
If your elbow pain comes with tingling in the pinky and ring fingers, don't guess. That pattern deserves a real evaluation, especially if you're trying to stay active in baseball, softball, lifting, dance, running, grappling, or court sports.
At PTU, we approach this the way athletes need it approached. We look at the nerve, the movement pattern, the training load, and the return-to-sport plan. That applies whether you're a high school athlete in Bridgewater, Massachusetts, an active adult from Plymouth or Taunton, a dancer from Raynham or East Bridgewater, or someone commuting from West Bridgewater, Buzzards Bay, or Middleborough.
If you're dealing with cubital tunnel syndrome elbow pain and want a sports-focused plan, start with an evaluation instead of waiting for the symptoms to “declare themselves.” A clear diagnosis early usually makes better decisions possible. For athletes who need broader performance rehab support, PTU also offers sports medicine and rehab services that fit return-to-play goals.
A licensed physical therapist should examine your individual case before you make decisions about treatment, training, or return to sport.
If elbow pain, finger numbness, or grip weakness is interfering with your training, book an evaluation with Physical Therapy U. PTU serves athletes and active adults across Southeastern Massachusetts with locations in Bridgewater, Buzzards Bay, and Middleborough, and the team can help you build a plan for recovery, performance, and safe return to sport.
{kind=link}