The most popular advice on ACL injuries still frames the decision the wrong way. People ask whether the ligament will heal on its own. Athletes should be asking a harder and more useful question: what can I safely get back to, at what level, and what signs tell me my knee isn't ready.
In sports physical therapy, that distinction matters. A runner in Bridgewater, Massachusetts, a soccer player in Plymouth, and a dancer on the South Shore don't just need less pain. They need a knee that can handle force, deceleration, position changes, and the mental load of trusting it again. That's why acl tear recovery without surgery isn't just a yes-or-no topic. It's a performance question.
If you're sorting through rehab options, nutrition support during recovery often comes up too. Supplements won't replace loading, strength work, or decision-making, but some athletes like to review trusted collagen brands as part of a broader recovery plan discussed with their clinician. For a deeper sports medicine discussion on how these decisions get made, PTU also has an ACL podcast episode with Dr. Eric Rightmire.
Table of Contents
- First Let's Redefine ACL Recovery
- Copers vs Non-Copers Who Can Succeed Without Surgery?
- The Phased Rehab Plan for Conservative ACL Recovery
- Advanced Return-to-Sport Training and Testing
- Outcomes Evidence and When to Reconsider Surgery
- FAQ Your Non-Surgical ACL Recovery Questions
First Let's Redefine ACL Recovery
A lot of athletes hear “ACL tear” and assume surgery is automatic. That's too simple. The better question is whether your knee can become functionally stable, strong, and reliable enough for your actual sport demands.
What recovery actually means
For athletes, recovery has several layers:
- Pain and swelling settle down
- Range of motion comes back
- Strength returns
- Movement quality improves
- The knee stops giving way
- Sport-specific confidence comes back
That's different from saying the ligament itself has fully restored normal structure. A review summarized by Cary Orthopaedics notes that the critical question isn't just “Will it heal?” but “What sport can I safely return to, at what level, and what instability signs mean I should stop?” It also notes that nonoperative care is most appropriate for partial tears and lower activity demands, and that a recent review found no certain evidence that ACL reconstruction is superior to well-designed nonoperative treatment for isolated ACL tears regarding osteoarthritis prevention, subjective outcome, or return to play, though reconstruction does provide better passive stability (Cary Orthopaedics on ACL healing without surgery).
Practical rule: Recovery without surgery is less about waiting for biology to save you and more about proving your knee can meet your sport's demands.
That changes the conversation. A cyclist, distance runner, and field sport athlete do not face the same decision. Neither do a middle school athlete, an adult recreational skier, and a collegiate lacrosse player.
Who usually fits nonoperative care
The athletes who tend to have the best chance with conservative management usually share a few traits:
- Their tear pattern is more favorable. Partial injuries tend to fit this path better than complete tears.
- Their knee is relatively quiet. Swelling settles, motion returns, and daily walking improves.
- They don't report repeated giving-way episodes. That matters a lot.
- Their sport demand is lower in cutting and pivoting. Straight-line activity is usually easier to tolerate than reactive change-of-direction sport.
- They're willing to train. This path is active. It is not passive rest.
For motivated athletes, that's often encouraging news. It also keeps expectations honest. You might recover very well for lifting, running, hiking, dance, or general training and still not be a good candidate for uncontrolled pivoting sport.
Copers vs Non-Copers Who Can Succeed Without Surgery?
Sports PTs often use a simple frame here. Some people become copers. Others are non-copers. The difference isn't toughness. It's whether the knee can stay stable under the loads and movement patterns that matter to that person.
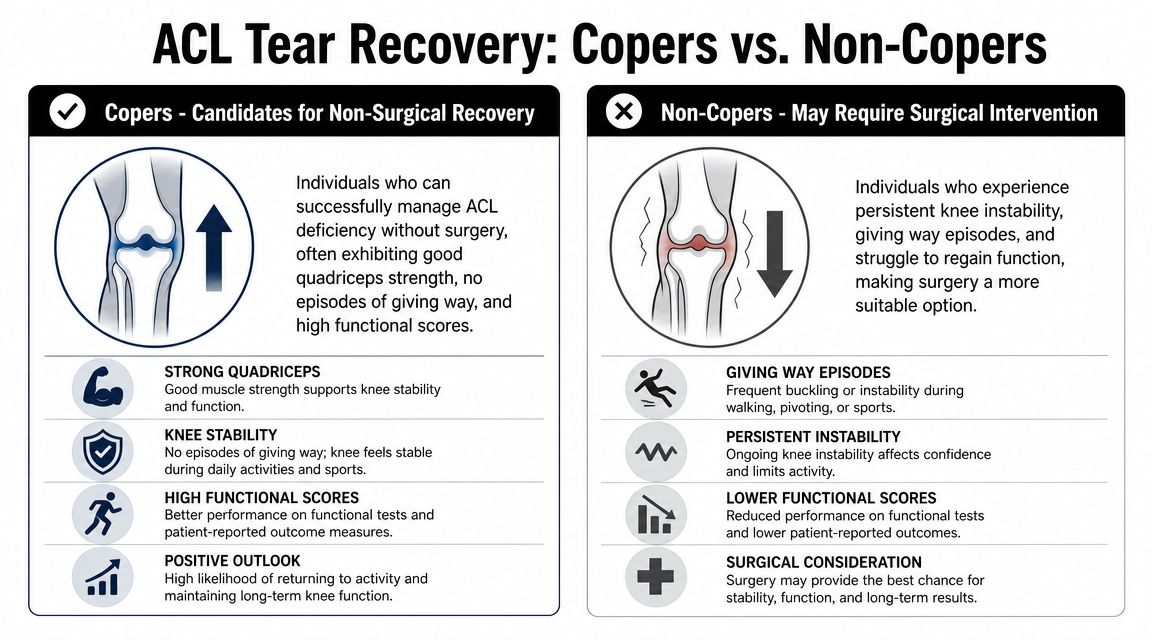
What makes someone a coper
A coper usually looks good in the clinic and in real life. Their swelling calms down, they regain motion, and their knee doesn't buckle during daily activity or progressive rehab.
Signs that support a nonoperative path include:
- No repeated instability episodes. If the knee isn't giving way, that's meaningful.
- Good strength recovery. Quads, hamstrings, and hip control matter.
- Strong single-leg control. They can own landings, deceleration, and balance tasks.
- Reasonable sport goals. Lower-demand or straight-line sports fit better.
- Clean decision-making. They don't rush back before fundamentals are ready.
What makes someone a non-coper
A non-coper usually tells you early. The knee keeps slipping. Direction changes feel sketchy. Cutting, pivoting, or even awkward daily movements trigger distrust.
The historical guidance from the MOON Knee ACL research summary is still clinically useful here. It states that although the knee may feel better after rehab, the torn ACL doesn't typically reattach, it becomes clear within 3–6 months whether adequate function can be achieved, persistent instability during that period often points toward reconstruction, and only a “tiny minority” are predicted to return to aggressive sports without surgery (MOON guidance on ACL rehab without surgery).
If your knee keeps giving way during ordinary rehab progressions, don't call that a confidence problem. Call it useful information.
That timeline matters in real decisions. An athlete in Taunton or Middleborough who wants to get back to basketball, soccer, football, or high-level field sport has to pay attention to instability early. Repeated episodes don't just delay progress. They usually tell you the current plan isn't enough for your goals.
A simple athlete filter
You're more likely to succeed without surgery if most of these are true:
- Partial tear
- No major instability symptoms
- No repeated buckling
- Sport doesn't depend on high-speed cutting and pivoting
- You can commit to structured rehab
- You're willing to modify activity while the knee earns more
You're less likely to succeed if several of these show up:
- Complete tear
- High-demand pivoting sport
- Multiple giving-way episodes
- Poor single-leg control
- You keep testing the knee before it's ready
That's not pessimistic. It's how good sports rehab protects long-term performance.
The Phased Rehab Plan for Conservative ACL Recovery
Nonoperative ACL rehab should be criterion-based, not calendar-based. UPMC's non-surgical guidance emphasizes controlling effusion and pain, restoring full knee extension, normalizing gait, and rebuilding strength before progressing, and it warns that moving into impact or pivoting too early raises the risk of instability episodes (UPMC non-surgical ACL rehab guidance).
Phase 1 calm the knee down
The first job is to make the knee less angry. If the joint is swollen, you can't extend fully, and your gait is altered, you don't have a real strength base yet.
Early priorities usually include:
- Settle swelling. Rest, ice, compression, elevation, and temporary offloading can help.
- Get full extension back. This is one of the most important early benchmarks.
- Normalize walking. Limping becomes a bad habit fast.
- Wake the quadriceps up. A quiet quad often drives poor control.
- Protect confidence. Early wins matter.
Common drills in this phase:
- Heel props or extension hangs
- Heel slides for flexion
- Quad sets
- Straight-leg raises when appropriate
- Gentle weight shifts
- Supported gait work
Full knee extension isn't a bonus milestone. It's foundational.
Phase 2 build strength you can trust
Once the knee is calmer and walking looks normal, the work gets more physical. Now you're building force production and load tolerance, not just checking boxes.
The main targets are the quadriceps, hamstrings, glutes, calf, and trunk. Athletes also need endurance here. A knee that looks good for one rep but falls apart under fatigue isn't ready for sport.
Examples of useful progressions:
- Closed-chain strength work. Squats, split squats, step-ups, and leg press variations.
- Posterior chain training. Bridges, Romanian deadlifts, hamstring curls, and hip hinge patterns.
- Single-leg basics. Supported split stance and progressive single-leg loading.
- Low-impact conditioning. Bike, pool, or similar options to rebuild work capacity.
If there's also meniscus irritation, rehab planning gets more nuanced. That's where related guidance on meniscus tear rehab without surgery can help frame what symptoms to watch.
Non-Operative ACL Rehab Phases & Goals
| Rehab Phase | Primary Goals | Example Activities |
|---|---|---|
| Early recovery | Reduce pain and effusion, regain full extension, normalize gait | Ice, compression, heel props, heel slides, quad sets, supported walking |
| Strength foundation | Build quadriceps, hamstring, glute, and calf strength | Squats, step-ups, bridges, leg press, bike conditioning |
| Control and progression | Improve balance, deceleration, and single-leg mechanics | Single-leg stance, step-downs, landing drills, controlled direction changes |
Phase 3 restore control under load
At this stage, many athletes think they're ready because pain is lower. They often aren't. The next layer is neuromuscular control under speed, fatigue, and asymmetrical loading.
Key elements here include:
- Single-leg balance with challenge
- Step-down control
- Landing mechanics
- Deceleration drills
- Lateral movement progressions
- Gradual running exposure if criteria are met
What doesn't work? Jumping from “I can squat” to “I can scrimmage.” That gap is where a lot of nonoperative ACL rehab fails.
A few mistakes show up over and over:
- Ignoring persistent loss of extension
- Progressing because time passed, not because function improved
- Returning to impact while swelling still rebounds
- Confusing a brace with readiness
- Skipping home loading because formal PT feels like enough
For athletes in Bridgewater, Buzzards Bay, and Middleborough, this criterion-based approach is the difference between random exercise and actual sports rehab. The knee has to earn each next step.
Advanced Return-to-Sport Training and Testing
Strength alone doesn't clear an athlete. The final stage is about whether you can absorb force, create force, and control the knee in the exact situations your sport demands.

Training the gap between rehab and sport
An athlete coming back without surgery often needs a long runway. One source discussing conservative recovery timelines notes that some protocols cite 8–10 weeks of supervised physical therapy just to regain enough function to handle sport or work demands, and 9–12 months for a cross-bracing-based return-to-sport pathway. It also stresses that success depends heavily on patient selection and not returning to cutting or pivoting too early (London Cartilage on ACL recovery timelines).
That shouldn't discourage you. It should sharpen the plan.
Advanced training usually includes:
- Plyometrics. Double-leg to single-leg jump and landing progressions.
- Deceleration training. Athletes get hurt slowing down as often as speeding up.
- Agility drills. Planned patterns first, reactive patterns later.
- Cutting mechanics. Introduced carefully, with control before chaos.
- Energy system work. Conditioning has to match the sport.
- Sport-specific skills. Ball handling, dance sequences, sprint mechanics, or position-specific movement.
For athletes comparing approaches from different providers, it can also help to review how other clinics discuss expert athletic injury care and progression standards. The useful part isn't the branding. It's seeing how consistently good sports rehab prioritizes criteria over guesswork.
What objective testing should show
Return-to-sport testing matters because confidence can lie. Objective data catches what motivation hides.
Useful benchmarks often include:
- Single-leg hop testing
- Landing quality on video
- Change-of-direction control
- Sprint mechanics
- Fatigue response
- Symptom response after higher-load sessions
At this level, added services can make a real difference. Running gait analysis can uncover compensations that don't show up in slower drills. Dance therapy matters when turnout, landing artistry, or repeated single-leg demand is part of the sport. Strength and conditioning fills the gap between rehab and true athletic capacity, which is why a structured strength and conditioning program for athletes is often part of the final build.
A short demo can help athletes visualize movement quality during this stage:
Return to sport is not the same as return to participation. Being able to join practice is different from being prepared for competition speed, contact, and fatigue.
For runners in East Bridgewater or West Bridgewater, that may mean restoring clean mechanics at faster paces before racing. For field and court athletes, it means proving the knee can tolerate cutting when the brain is busy and the body is tired.
Outcomes Evidence and When to Reconsider Surgery
The evidence on nonoperative ACL care is more nuanced than many athletes expect. It doesn't support the idea that surgery is mandatory for everyone. It also doesn't support pretending that all knees do equally well without reconstruction.
What the evidence actually supports
A systematic clinical report on ACL healing found that spontaneous healing was observed in 14% of patients overall. The strongest signal appeared in a narrow subgroup, especially partial ACL ruptures with favorable characteristics. Even then, “healed” did not mean normal. Midterm knee function could be satisfactory, but stability remained reduced compared with the uninjured side and activity scores were lower than pre-injury levels.
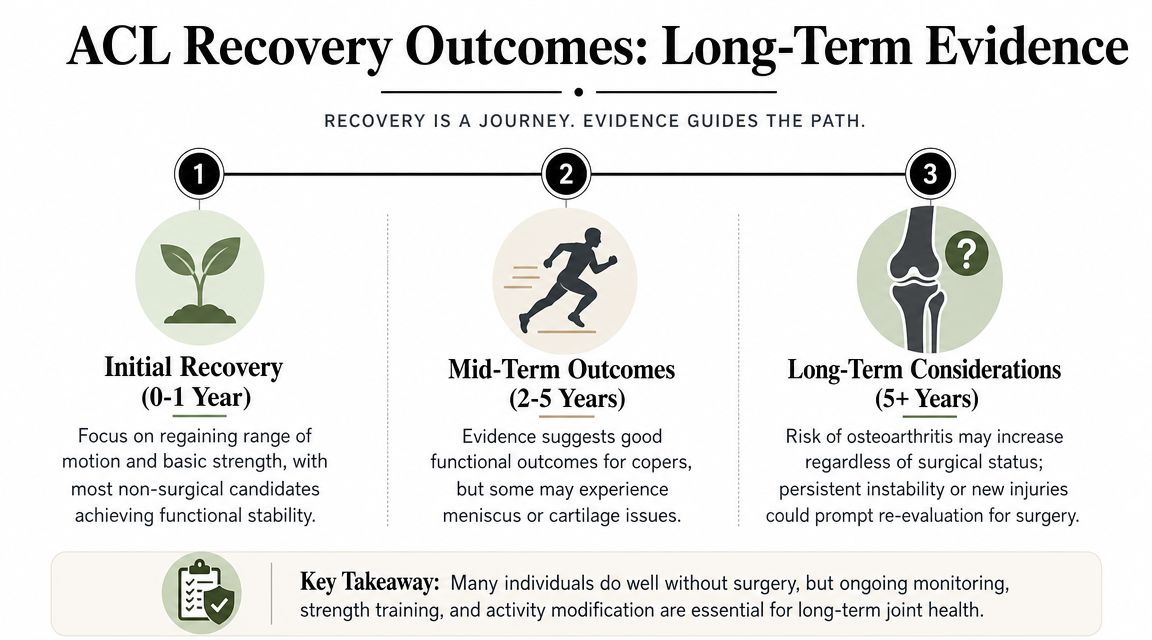
That's the key trade-off. Acl tear recovery without surgery is usually about functional compensation, not full biologic restoration. Some athletes do very well with that. Others hit a ceiling because their sport asks more of the knee than compensation can safely provide.
Red flags that change the plan
The athletes who should reconsider surgery usually don't need convincing. Their knee keeps sending the message.
Watch for these signs:
- Repeated giving-way episodes
- Swelling that returns with progression
- Persistent pain that limits loading
- Inability to advance into running, jumping, or directional work
- Loss of trust in the knee during normal sport tasks
- A mismatch between your goal sport and the stability you can demonstrate
When the knee repeatedly fails the demands you care about, the plan has to change. Sticking with conservative care out of stubbornness isn't the same as giving rehab enough time.
A skilled re-evaluation matters. In the South Shore Massachusetts area, that often means a sports PT and orthopedic surgeon should both be part of the conversation. The decision isn't “Did rehab fail?” Sometimes rehab worked exactly as intended. It clarified that your daily life is manageable, but your goal sport still requires more passive stability than your knee can provide.
FAQ Your Non-Surgical ACL Recovery Questions
Can I play soccer or basketball again without surgery
Maybe, but that's the hardest category. Sports with frequent cutting, pivoting, and reactive contact place the biggest demand on an ACL-deficient knee. Some athletes can function well nonoperatively, but high-demand pivoting sport is where expectations need to be strict and testing needs to be objective.
A better question is whether you can demonstrate stable deceleration, single-leg control, change-of-direction tolerance, and no giving-way episodes as training advances. If those don't show up, the answer is usually no, or not yet.
Should I wear a brace
A brace can be useful in some cases, especially early or during specific higher-risk drills. It may improve confidence and provide some external support, but it doesn't replace strength, control, or good decision-making.
The mistake is relying on the brace as proof that the knee is ready. Under-bracing can leave some athletes feeling exposed. Over-bracing can create false confidence and delay proper loading. The right choice depends on your symptoms, sport, and exam findings.
Can dry needling help during ACL rehab
Sometimes, yes. Dry needling doesn't heal the ACL itself, but it can be helpful when surrounding tissues get overloaded during rehab. Athletes often develop calf, quad, hamstring, or hip tightness as they compensate.
In a sports PT setting, dry needling is best used as an adjunct. It can reduce muscular guarding and improve tolerance to movement, but it should sit next to strength work, progressive loading, and movement retraining. It shouldn't become the main event.
How do I know if my tear is partial or complete
That usually requires imaging and an orthopedic evaluation, along with a hands-on exam. The rehab presentation matters too. A knee with better early stability and fewer giving-way episodes may fit the profile of a more favorable injury pattern, but you can't confirm tear type by symptoms alone.
If you're unsure, get assessed by a licensed physical therapist and the appropriate medical specialist. That's especially important if you're a youth athlete, a parent trying to make decisions for a teen athlete, or an adult trying to return to cutting sport.
Can I still run without surgery
Often, yes, but not immediately and not by guesswork. Running has lower rotational demand than many field and court sports, but it still requires force acceptance, leg stiffness, rhythm, and confidence.
Most athletes should earn running through criteria. You want quiet swelling, full extension, strong enough single-leg control, and a gait pattern that doesn't shift load poorly. Running gait analysis can be especially useful here because subtle compensation can hide until pace increases.
What if I feel good but still don't trust the knee
That's common, and it matters. Pain relief and trust are not the same thing. Some athletes feel fine in the gym and then freeze during a cut, landing, or unplanned direction change.
That gap is exactly why return-to-sport testing exists. The answer usually isn't “push through it.” The answer is to identify whether the problem is strength, movement quality, exposure to higher-speed tasks, or genuine instability.
When should I stop trying conservative care
Stop and get re-evaluated if the knee keeps giving way, swelling returns each time you progress, or you stall despite doing the work. Also get rechecked if your goal is a high-demand pivoting sport and your knee still can't tolerate the training needed to prepare for it.
That doesn't mean you did anything wrong. It means the decision has become clearer.
If you're dealing with an ACL injury and want a sport-specific plan instead of generic knee rehab, book an evaluation with Physical Therapy U. Our licensed DPT team works with athletes, runners, dancers, and active adults across Bridgewater, Buzzards Bay, and Middleborough, with return-to-sport testing, running gait analysis, dry needling, dance therapy, and performance-based rehab designed around what you want to get back to.
{kind=link}