You're probably here because running has started to feel less reliable than it should.
Maybe your knee tightens up every time you add mileage. Maybe your shin settles down for a week, then lights up again on the next long run. Maybe your hip aches after trail runs near Taunton, or you're training for a race in Plymouth and can't shake the feeling that something in your stride is off. Rest helps, then it doesn't. New shoes help, then they don't either.
That's usually the point where a runner needs more than general advice. In sports physical therapy, running gait analysis helps connect the pain you feel to the movement pattern creating it. Instead of guessing whether the problem is your foot, your shoes, your training load, or your strength, we look at how your whole system handles force while you run.
Table of Contents
- That Nagging Injury That Just Won't Go Away
- What Is Running Gait Analysis Really Measuring
- The Tools We Use to Analyze Your Running Form
- Common Gait Findings and What They Mean for You
- Your Gait Analysis Appointment at PTU What to Expect
- From Analysis to Action How We Build Your Recovery Plan
- Frequently Asked Questions About Running Gait Analysis
That Nagging Injury That Just Won't Go Away
A common sports PT story goes like this. A runner from the South Shore builds training steadily, feels strong for a few weeks, then gets the same pain in the same place. They back off, stretch more, ice it, maybe swap shoes, then restart and end up right back where they began.
That loop is frustrating because it feels like the body is being unpredictable. Most of the time, it isn't. The body is repeating the same loading pattern, and the same tissue keeps paying for it.

In a sports-focused clinic, the first question isn't just “where does it hurt?” It's “what happens when you run?” Pain that shows up at mile three, on downhills, during speed work, or only after hills gives useful clues. So does a history of ankle sprains, past ACL surgery, or a recent jump in training.
Why recurring pain usually needs a movement answer
A lot of runners assume the painful spot is the source of the problem. Sometimes it is. Often it's the area absorbing stress created somewhere else.
A sore knee may reflect what the hip isn't controlling well. A stubborn shin may relate to how the foot contacts the ground or how far the leg reaches in front of the body. An irritated hip may be dealing with trunk control problems that show up only under running load.
Practical rule: If pain keeps returning when training returns, the issue usually needs more than rest.
That's where running gait analysis becomes useful. It gives you a way to stop arguing with symptoms and start identifying the pattern underneath them.
What runners usually want, and what matters clinically
Most runners don't come in asking for biomechanical terminology. They want to run without limping through the week, train for a PR, or get through a season without another setback.
Clinically, that means the analysis has to answer real questions:
- Pain reduction: Which movement pattern is most likely increasing stress on the irritated area?
- Performance carryover: Is your form costing you rhythm, efficiency, or confidence at faster paces?
- Training decisions: Can you keep running while fixing the issue, or do you need a temporary modification?
- Durability: Which changes are likely to stick once race season gets busy again?
Good gait analysis doesn't just label your form. It gives your rehab a direction.
What Is Running Gait Analysis Really Measuring
A clinical running gait analysis is not the same as someone watching you jog for a few seconds and telling you whether you heel strike. It's a biomechanical assessment of how your body absorbs force, controls motion, and produces propulsion from one step to the next.
One useful way to think about it is as a diagnostic scan for your running engine. If a car pulls to one side, you don't only inspect one tire. You look at alignment, suspension, loading, and how the whole system works together. Running works the same way.
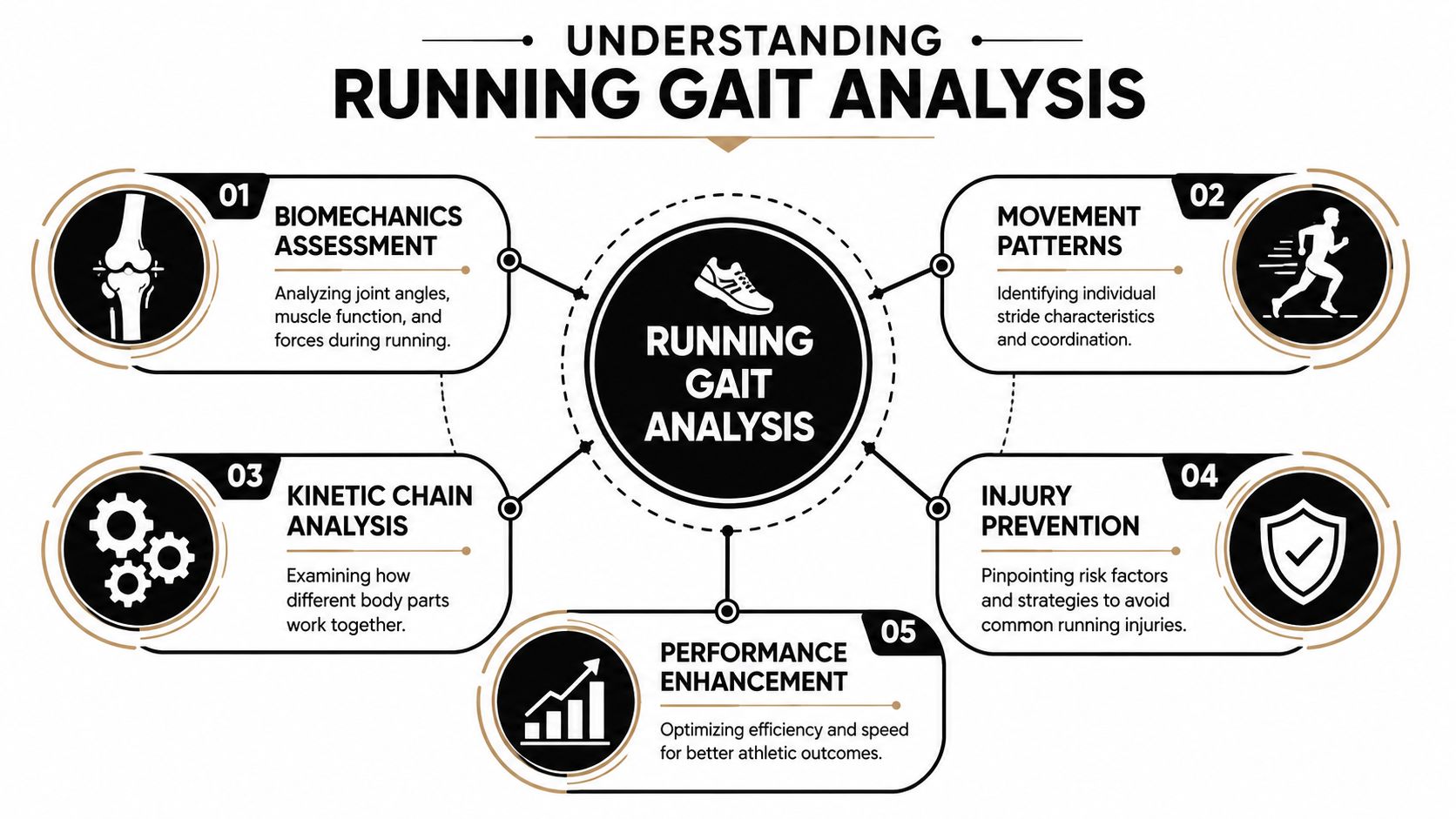
It's a whole-body movement assessment
Clinical gait analysis typically measures stride length, cadence, foot strike pattern, ground reaction forces, and joint alignment, and it evaluates more than the foot alone. Standard assessment also looks at at least one full gait cycle, meaning one foot strike to the next foot strike of the same foot. Many clinical protocols recommend high-speed video at 60 frames per second or higher from the side, back, and front so the clinician can accurately assess trunk, arm, hip, knee, and ankle motion, as described in this peer-reviewed overview of clinical gait analysis.
That matters because runners don't move in isolated parts. Your ankle position affects your knee. Your trunk position changes how your hip works. Your arm swing can alter timing and rotation. A gait analysis looks at those links, not just the final symptom.
A few of the things we care about most are:
- Step timing: Is your rhythm efficient, or are you spending too long on each contact?
- Landing position: Is the foot landing under you, or too far out front?
- Joint control: Do the hip and knee stay organized through stance, or drift into collapse?
- Force management: Are you loading smoothly, or slamming into the ground and asking irritated tissue to absorb too much?
Here's a quick visual overview before we go deeper into tools and findings.
Why video alone isn't enough
Slow-motion video is useful, but a clinical analysis doesn't stop there. The runner's injury history, symptom behavior, training goals, and off-treadmill exam all shape what the video means.
For example, two runners may show a similar landing pattern. One has no pain and excellent control. The other has patellofemoral pain and poor single-leg strength. The same visual can lead to a different plan because the context is different.
A gait finding only matters if it explains the problem you're trying to solve.
That's why a proper analysis links mechanics to your real goal. Maybe the goal is less knee pain on downhills. Maybe it's building confidence after surgery. Maybe it's running your next local race feeling smoother at faster paces. The numbers and video are only useful if they help us make that next decision.
The Tools We Use to Analyze Your Running Form
Technology helps. It also gets overvalued.
The best running gait analysis uses equipment to make subtle movement visible and measurable, but the equipment doesn't do the clinical reasoning for you. A treadmill, camera, sensor, or force system can capture data. A sports physical therapist has to decide what that data means, what to ignore, and what to change first.
2D video analysis
This is the workhorse in most clinical running assessments. High-speed cameras let us slow your stride down frame by frame so we can study how your trunk, pelvis, hip, knee, and foot move at key moments.
From the side view, we can inspect where your foot lands relative to your body and whether your posture supports efficient movement. From the rear view, we can look for pelvic drop, knee position, and how the foot behaves during stance. The front view can help confirm asymmetry and overall control.
2D video is especially helpful because runners often can't feel what they're doing. They may swear they're landing softly or staying level through the hips, then the slowed footage shows a very different story.
Wearable data
Wearables add objective feedback to what the eye sees. The most common value is rhythm and timing data, especially cadence. Some runners also like seeing real-time cues on a running watch because it helps them practice changes outside the clinic.
If you train with a GPS watch, comfort matters more than people think. A loose band shifts, irritates the wrist, or makes you stop paying attention to the data. If you use a Garmin Forerunner, durable Forerunner watch bands can be a practical upgrade when you're doing repeated treadmill work, sweat-heavy sessions, or longer outdoor runs.
Wearables are useful for:
- Cadence tracking: Easy to monitor during gait retraining.
- Session-to-session consistency: Helpful when you're trying to hold a new rhythm under fatigue.
- Feedback outside the clinic: Lets runners practice without guessing.
Force data in higher-need cases
In more advanced setups, force plates or instrumented treadmills show how the body interacts with the ground. That can be especially useful when a runner's symptoms are stubborn, speed-dependent, or not well explained by basic video alone.
Force data doesn't replace clinical judgment. It adds another layer. If someone reports pain only at faster paces, the loading pattern may not appear until we test under those conditions. Modern clinical gait analysis often combines treadmill running with force plates and video cameras so movement and force production can be assessed in real time while the athlete runs at a preferred speed or faster if needed, as noted in the earlier research overview.
Clinic reality: Better tools don't always mean a better plan. Better interpretation does.
A flashy report can still miss the point if it doesn't account for your strength, mobility, surgery history, training load, or race goals. The right question isn't “what tech do you use?” It's “how does this change the treatment plan?”
Common Gait Findings and What They Mean for You
Most runners don't need a long list of everything that looks imperfect. They need the few findings that relate to symptoms, workload, and performance.
Some gait patterns are worth changing. Some are normal variation. The clinical skill is knowing the difference.
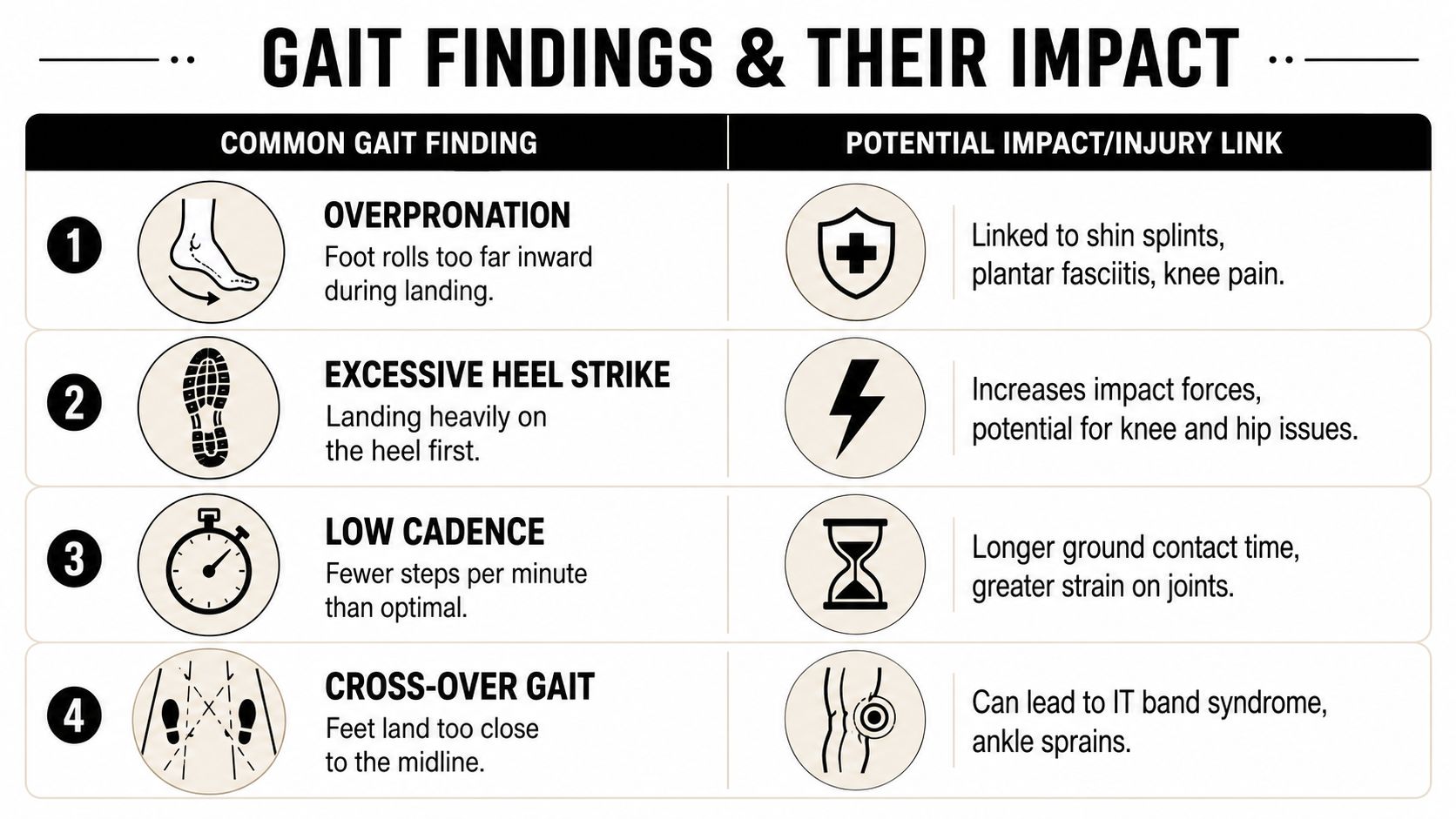
Overstriding
Overstriding usually shows up when the foot lands too far in front of the body. On video, it often looks like the runner is reaching for the ground instead of letting the body travel over the foot.
That tends to create a braking pattern. The leg is out in front, the knee takes more of the initial load, and the stride can sound louder and look harsher.
Common complaints that fit this pattern include:
- Front-of-knee pain: Often aggravated by downhills or faster running.
- Shin symptoms: Especially when contact feels abrupt.
- Hip irritation: The body may compensate upstream to handle repeated braking.
Low cadence
Cadence is one of the cleaner, more actionable findings in running rehab. Clinical guidance often places elite runners around 180 steps per minute, while recreational runners are commonly advised to aim for 160+ steps per minute. Ohio State Sports Medicine also notes that increasing cadence by 5% to 10% can substantially reduce forces on the hips and knees in runners with an injury history, which is why cadence is such a useful intervention target in practice, according to Ohio State Sports Medicine's running gait guidance.
A low step rate often pairs with overstriding, but not always. Some runners spend too long on each step and overload the same tissues repeatedly.
If cadence is part of the problem, the fix usually isn't “run faster.” It's a small rhythm adjustment that helps shorten the stride and smooth out loading.
Small cadence changes can make a big difference because they alter how often and how hard you load the same joint.
If a runner needs broader support around strength, mechanics, and training structure, a well-built strength and conditioning program for athletes can reinforce the gait changes instead of leaving them as treadmill-only cues.
Knee collapse and pelvic drop
Dynamic knee valgus means the knee drifts inward during stance. Pelvic drop shows up when the opposite side of the pelvis drops instead of staying controlled. Runners often notice neither, but the camera catches both quickly.
These findings often point toward problems with hip strength, trunk control, or single-leg stability, which are commonly observed in runners with patellofemoral pain, lateral knee irritation, or a general sense that one side feels less stable than the other.
On video, this can look like:
| Finding | What you see | What it may suggest |
|---|---|---|
| Knee valgus | Knee falls inward during loading | Reduced hip control or poor single-leg stability |
| Pelvic drop | Opposite hip dips in stance | Glute and trunk control deficits |
| Uneven side-to-side motion | One leg looks less organized | Compensation from prior injury or weakness |
Cross-over and foot control issues
Some runners land with the feet too close to the midline. That cross-over pattern can narrow the base of support and increase rotational stress up the chain. Others show foot mechanics that are less about the foot itself and more about what the hip and trunk are forcing the foot to manage.
Oversimplified advice causes trouble. A runner may hear “you overpronate” and assume the shoe is the whole answer. Sometimes footwear helps. Sometimes the more important fix is improving control higher up the chain so the foot doesn't have to overwork.
The point of running gait analysis isn't to make every runner look the same. It's to identify which findings are driving pain or limiting performance, then act on those first.
Your Gait Analysis Appointment at PTU What to Expect
Most runners are more comfortable once they know the process. A clinical running gait analysis is straightforward, and it feels much more like a sports evaluation than a generic rehab visit.
Come in wearing your normal running clothes and bring the shoes you train in. If you rotate shoes, bring the pair you use most often or the pair that seems tied to symptoms.
The conversation
The session starts with history. We ask about your training, recent mileage changes, surfaces, workout types, race goals, and exactly when symptoms show up.
That detail matters. Pain during tempo work is a different problem from pain that appears only the next morning. A runner returning after ACL rehab has a different loading story than a high school athlete trying to get through preseason conditioning in Bridgewater, Massachusetts.
The physical exam
The treadmill is only part of the story. Before anyone analyzes your stride, a sports PT should look at strength, mobility, balance, control, and movement quality off the treadmill.
That exam often includes single-leg tasks, hip strength assessment, ankle mobility, and checks for side-to-side differences that may explain what the running video later shows. It's also where we separate a running form issue from a tissue capacity issue, because sometimes the movement is only part of the problem.
If pain is limiting training tolerance, some runners also benefit from pairing rehab with symptom-management tools such as laser therapy for targeted pain and tissue support, depending on the presentation.
The treadmill review
Once you run, the goal isn't to force a perfect-looking stride. It's to capture your normal pattern. In knee-load-focused analysis, three especially actionable 2D measures are foot inclination at initial contact, peak knee angle at mid-stance, and step rate (cadence). Clinical teaching in this area also treats cadence as highly modifiable, which makes it a practical target when the goal is reducing knee force without making the runner feel unnatural, as outlined in this expert lecture on knee-load-focused gait analysis.
You'll usually review the footage with the therapist rather than getting a vague summary. That's important. When runners can see the pattern themselves, cues make more sense and changes stick better.
A useful appointment usually ends with clear answers to these questions:
- What are the main findings?
- Which of them matter for my pain or performance?
- What should I change first?
- Can I keep running while I work on it?
That clarity is what turns an assessment into a plan.
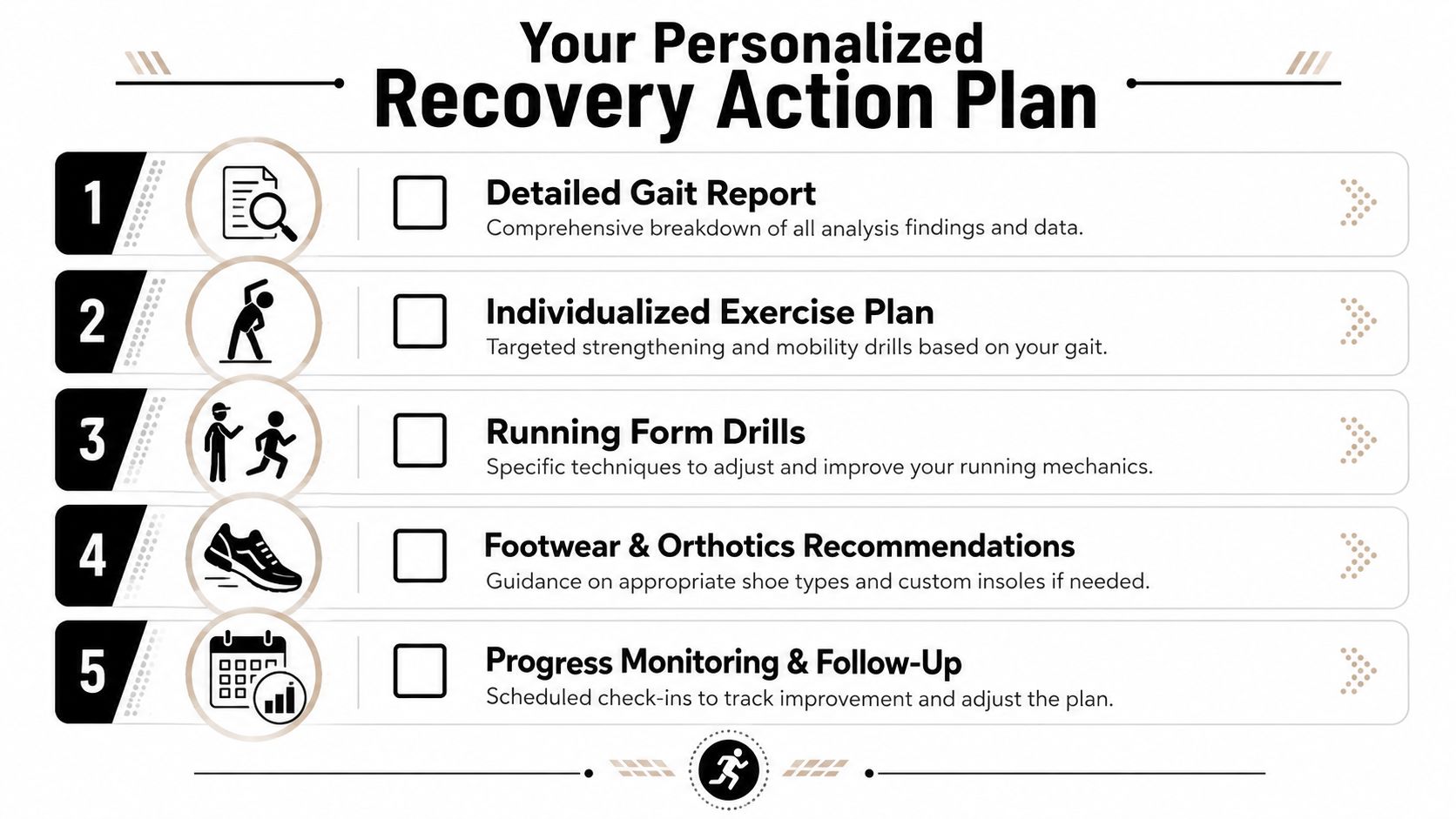
From Analysis to Action How We Build Your Recovery Plan
A gait report by itself doesn't fix anything.
What matters is whether the finding changes what you do this week, this month, and over the next training block. Good sports PT uses gait analysis to narrow the plan down to a few high-value changes, not to hand you a list of flaws.
What actually changes after the test
Neutral clinical guidance on gait analysis makes an important point. Yes, it can detect asymmetries and movement patterns, but the key value comes from deciding when findings are actionable and which interventions should be prioritized for durable outcomes, especially in the context of the runner's injury history, as discussed in this clinical perspective on whether gait analysis improves running form.
That lines up with what works in practice. Not every visible asymmetry needs to be corrected. Not every runner with pain needs a major form overhaul. Often the best plan is a modest gait cue, a strength progression, and a smart return-to-run structure.
Change the pattern that changes the load. Leave the rest alone unless it becomes relevant.
Examples of how the plan gets built
Here's what that might look like after a running gait analysis:
- For overstriding or harsh landing: We may use cues like “shorter steps” or “run quieter,” then rehearse them at controlled paces.
- For pelvic drop or poor single-leg control: The plan often includes glute and trunk work, then drills that carry that control into actual running.
- For recurrent knee irritation: We may prioritize cadence work, hip control, and surface or workout modifications before changing anything else.
- For post-injury return: We match running volume to tissue tolerance, not just motivation.
Exercise selection should be specific. A runner with pelvic drop might get:
- Hip bridge variations: To build posterior chain support.
- Side-lying or standing hip work: To improve lateral hip control.
- Single-leg balance and step-down patterns: To carry strength into stance control.
- Core stability drills: To reduce unnecessary trunk motion.
A broader home program can build on these priorities, especially when paired with a structured set of physical therapy exercises for runners that target strength, mobility, and control.
Recovery habits matter too, especially during harder training blocks. For runners who want a practical overview of nutrition support, this guide to optimize your recovery with supplements can be a helpful general resource alongside your rehab plan.
In some cases, we also layer in hands-on treatment, dry needling, or mobility work if the runner has restrictions that make the new movement pattern hard to access. Then we build a return-to-run progression that lets the body practice the new mechanics under manageable load.
That's the difference between spotting a problem and solving it.
Frequently Asked Questions About Running Gait Analysis
Do I have to be injured to get a gait analysis
No. Plenty of runners use running gait analysis for performance, efficiency, or to prepare for a race block. It's also useful if you're new to running and want a cleaner starting point before mileage builds up.
What's the difference between this and a running store analysis
A store analysis may help with footwear decisions. A clinical analysis adds a musculoskeletal exam, injury-history review, movement testing, and a rehab plan if something is off. That's a different level of decision-making.
Is it covered by insurance
In many cases, runners receive gait analysis as part of a physical therapy evaluation, which is often covered by major insurance plans. Coverage varies by plan, so it's worth verifying benefits before the visit.
How long does it take to notice results
That depends on the problem, how long symptoms have been present, and whether the issue is mostly movement-based, strength-based, or both. Some runners feel a difference quickly with the right cue. Others need a longer progression to make the change durable.
What should I bring to the appointment
Bring your usual running shoes, running clothes, and any recent shoe pair that seems tied to symptoms. If you use audio cues or metronome work during runs, comfort matters there too. Runners comparing options for training audio may find Back Bay Brand's JBL earbuds analysis useful when choosing gear for treadmill sessions and outdoor workouts.
If you're tired of guessing why running still hurts, book an evaluation with Physical Therapy U. PTU is an athlete-centered sports physical therapy clinic serving Southeastern Massachusetts with locations in Bridgewater, Buzzards Bay, and Middleborough. If you're in Bridgewater, Massachusetts, or nearby towns like Plymouth, Taunton, East Bridgewater, West Bridgewater, Raynham, or across the South Shore Massachusetts area, the team can help you connect your running form to a clear rehab and performance plan.
{kind=link}