You tweak your stride because your knee hurts on cutbacks. Your shoulder feels loose after a weekend baseball game. Your dancer says their ankle is “fine,” but they're still avoiding landings. Most athletes don't need another vague instruction to rest and hope. They need a plan.
That's where sports medicine and rehab should feel different. It isn't just treatment for pain. It's a structured process that connects diagnosis, movement analysis, strength work, recovery, and return-to-sport testing so you know what to do next and why you're doing it.
That matters because sports injuries are common. In the U.S., over 3.5 million sports injuries occur annually among 30 million participants according to Grand View Research's sports medicine industry overview. For athletes in Bridgewater, Massachusetts, Buzzards Bay, Middleborough, Plymouth, Taunton, East Bridgewater, West Bridgewater, and Raynham, the central question usually isn't “Do I need help?” It's “How do I get back without making this worse?”
Table of Contents
- Your Guide to Sports Medicine and Rehab at PTU
- What to Expect During Your Initial Evaluation
- The Four Phases of Athlete Rehabilitation
- Evidence-Based Treatments That Accelerate Recovery
- Sport-Specific and Population-Specific Programs
- Return-to-Sport Testing and Measuring Success
- Frequently Asked Questions About Sports Rehab
Your Guide to Sports Medicine and Rehab at PTU
An athlete usually shows up with two problems. The first is the injury. The second is uncertainty. They don't know whether they should shut it down, push through, lift around it, or get imaging first.
A good sports rehab process answers those questions quickly. It treats the pain in front of you, but it also looks at the training errors, movement deficits, stiffness, weakness, or force-control issues that helped the problem build in the first place. That's the difference between getting through a season and restoring performance.
At an athlete-centered clinic, rehab isn't passive. You're not there to collect a sheet of generic exercises and count the days until you're “cleared.” You're there to work with a doctor of physical therapy who can match the plan to your sport, your position, your schedule, and your current capacity.
That matters whether you're a middle school soccer player from Taunton, a runner on the South Shore Massachusetts roads, a high school basketball athlete in Plymouth, or an adult lifting again after knee surgery.
Practical rule: The best rehab plan doesn't just reduce symptoms. It gives you objective reasons to trust your body again.
Sports medicine and rehab also needs to reflect real life. Some athletes need dry needling because a painful calf won't let them load. Some need running gait analysis because the pain keeps returning. Some dancers need a program built around turnout demands, landing control, and repetitive volume. Some post-op patients need a longer runway and stricter testing before practice even becomes an option.
The common thread is simple. Progress should be earned, not assumed.
What to Expect During Your Initial Evaluation
Your first visit should feel less like a generic medical appointment and more like the start of a training partnership. If the evaluation is rushed, the plan usually gets rushed too.
The conversation comes first
The first part is a detailed history. We want the timeline, the training load, the aggravating movements, what you've already tried, and what you need to get back to. “My knee hurts” isn't enough. We need to know if it hurts on deceleration, on stairs, after long runs, only during cutting, or only the next morning.
We also ask about your sport background because the same body part can mean very different things in different athletes. Shoulder pain in a baseball player, swimmer, and dancer doesn't behave the same way. An ankle issue in a lineman, point guard, and ballet dancer won't be managed the same way either.
Questions that matter often include:
- Training details: What does a normal week look like, and what changed before the pain started?
- Sport demands: Do you need sprinting, jumping, rotation, overhead power, deep squatting, pointe work, or long-distance volume?
- Recovery picture: Are you sleeping well, managing soreness, and tolerating practice loads?
- Goal clarity: Is the target daily comfort, offseason training, opening day, or safe return after surgery?
The movement assessment finds the missing piece
After the conversation, the physical assessment starts. This includes range of motion, strength testing, palpation when useful, balance, gait, jump mechanics, and sport-specific movement screens.
The “why” is important. Pain is only part of the story. If your hip can't extend, your calf doesn't absorb force, or your trunk control collapses on one leg, the painful area may be doing extra work every time you train. That's how people get stuck in the cycle of “better for a week, worse after practice.”
A thorough evaluation often looks at:
- Mobility: Joint motion, muscle length, and whether stiffness is changing movement quality.
- Strength: Not just whether a muscle can fire, but whether it can produce and control force.
- Movement strategy: Squats, hops, step-downs, cutting mechanics, landing quality, and running form.
- Irritability: How easily the injury flares, and how much loading it can tolerate right now.
The first visit should leave you with a clearer map, not more confusion.
By the end of the evaluation, the rehab plan should make sense to you. You should know what tissue or movement problem is most likely involved, what you can keep doing, what needs to change temporarily, and what milestones matter next. That's how rehab becomes specific instead of reactive.
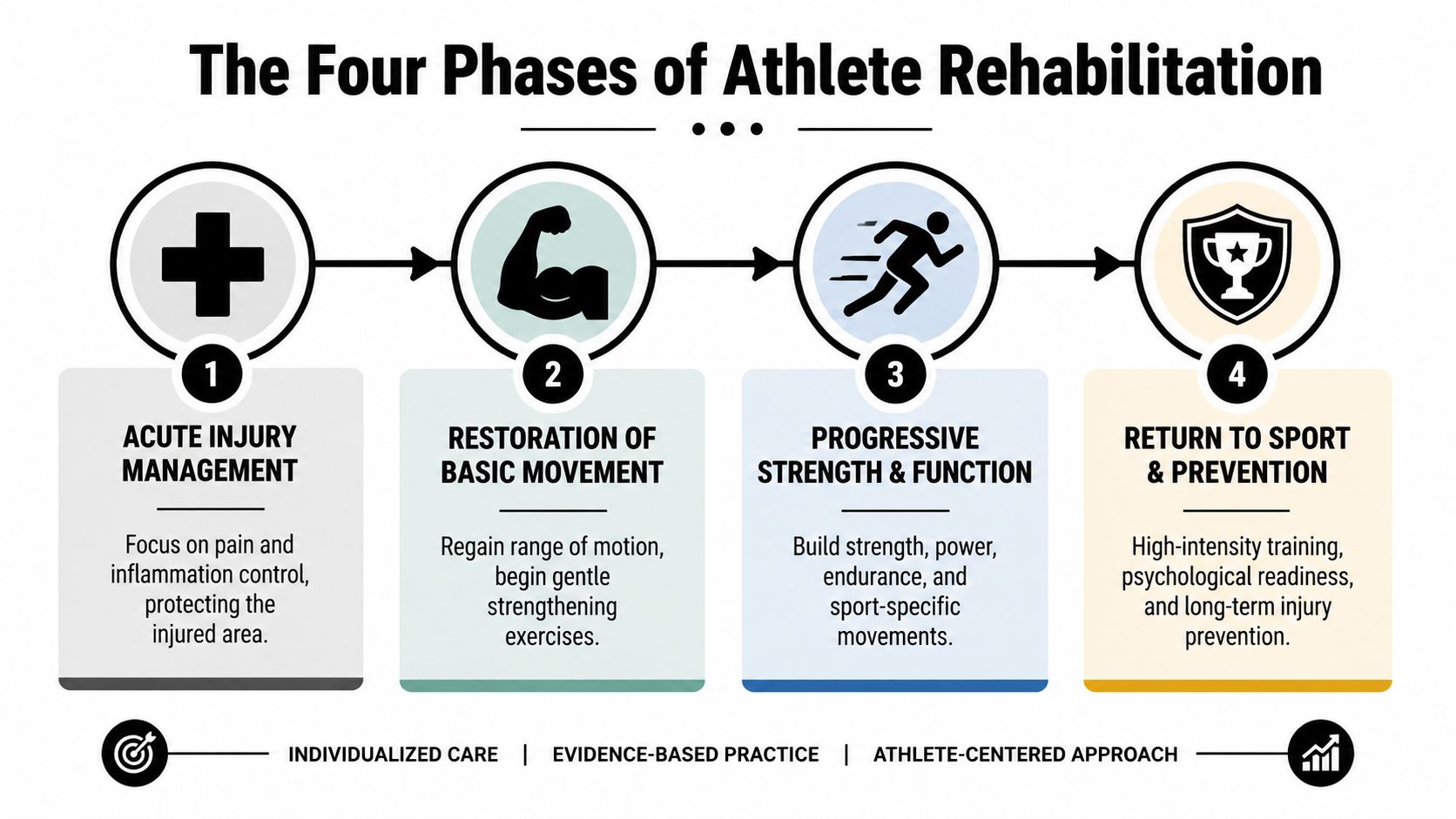
The Four Phases of Athlete Rehabilitation
Most athletes have heard some version of “give it six weeks.” That's not how strong rehab works. Time matters, especially after surgery, but criteria matter more because bodies don't all recover on the same schedule.
Early on, many athletes are dealing with the most common injury bucket. Sprains and strains account for about 30% of all sports injuries according to Market.us sports medicine statistics. That's one reason the first phase of rehab is often about calming symptoms without losing too much capacity.
Phase 1 and Phase 2
Phase 1 is pain and inflammation control. The goal isn't complete rest unless protection is necessary. The goal is to reduce irritation, protect the injured area, and keep the rest of the body moving.
Typical Phase 1 work may include:
- Load modification: Reduce cutting, jumping, mileage, or lifting depth so the tissue can settle.
- Protected motion: Gentle mobility drills that prevent stiffness without provoking symptoms.
- Isometrics or low-load activation: Early muscle work to maintain connection and tolerance.
- Recovery support: Compression, manual therapy, and activity changes that help symptoms calm down.
Phase 2 restores motion and basic strength. Pain is no longer the only priority. Now the focus shifts to regaining clean movement patterns and rebuilding foundational force production.
What tends to work here:
- Range of motion drills: Joint and soft tissue mobility where restriction is limiting movement.
- Foundational strength: Split squats, bridges, calf raises, rows, presses, or controlled bodyweight patterns.
- Balance and control: Single-leg stability, tempo work, and positional awareness.
- Technique retraining: Better squat, landing, or gait mechanics before adding intensity.
| Phase | Primary Goal | Example Activities | Criteria to Advance |
|---|---|---|---|
| Phase 1 | Calm symptoms and protect tissue | Load modification, gentle mobility, isometrics, recovery work | Pain is more manageable and basic movement is tolerated |
| Phase 2 | Restore motion and base strength | Mobility drills, controlled strength work, balance training | Movement quality improves and everyday loading is better tolerated |
| Phase 3 | Build sport capacity | Plyometrics, heavier strength work, deceleration, change of direction | Athlete handles higher force and more complex movement well |
| Phase 4 | Return to sport safely | Testing, high-speed drills, practice progressions, prevention work | Objective benchmarks and sport demands are met |
For athletes dealing with cartilage or knee symptoms that don't always require surgery, this overview of meniscus tear rehab without surgery is a useful example of how symptom control and progressive loading fit together.
Phase 3 and Phase 4
Phase 3 builds strength, power, and sport function. At this stage, rehab starts to look more like training again. The athlete needs enough tissue tolerance to handle speed, impact, and repeated effort.
That often includes:
- Progressive strength training: Heavier split squats, deadlift patterns, step-down variations, and unilateral loading.
- Rate of force development: Jumps, skips, med ball drills, and faster concentric work when appropriate.
- Deceleration practice: Landing mechanics, stick work, and controlled cutting.
- Conditioning: Rebuilding the engine so fatigue doesn't wreck mechanics late in practice.
Phase 4 is return to sport and prevention. This phase is where many athletes want to rush, and it's also where shortcuts create setbacks. If a basketball player can squat but can't absorb force on one leg, react to direction changes, and trust that movement under pressure, they're not ready.
Rehab isn't finished when pain is gone. It's finished when the body can meet the demands of the sport again.
Phase 4 blends objective testing, practice exposure, and ongoing strength work. The athlete earns progression by showing they can do the next thing well, not by reaching a date on the calendar.
Evidence-Based Treatments That Accelerate Recovery
Athletes often ask which treatment works fastest. The better question is which treatment fits the problem in front of you. The right tool can help, but no tool can replace a good loading plan.

What each tool actually does
Manual therapy is useful when stiffness, pain, or guarding is limiting movement quality. Joint mobilization and soft tissue work can create a short-term window for better motion. That window matters only if you use it right away with exercise, strength work, or motor retraining.
Dry needling can help reduce muscle tone, trigger point irritability, and protective guarding in the right athlete. It's often most helpful when a calf, quad, hip, shoulder, or forearm is staying “on” and blocking good movement. It's not magic, and it's not the whole plan. It's a way to make the next phase of movement more available.
Laser therapy is typically used when tissue healing support and symptom reduction would help the athlete tolerate loading better. It fits best when paired with a plan that still asks the body to adapt instead of waiting passively.
Later in the session, athletes often benefit from seeing exercise choices in motion, especially when they're trying to understand why one drill is prescribed over another.
What works and what doesn't
NormaTec compression and recovery sessions can be useful for soreness management, circulation support, and helping athletes tolerate higher training frequencies. These tools are especially practical during intense return-to-running or return-to-practice periods when the athlete is loading hard enough to need structured recovery.
What tends to work well in sports medicine and rehab:
- Pairing treatment with exercise: Soft tissue work followed by movement retraining.
- Choosing tools for a reason: Dry needling for a guarded muscle, not because it's trendy.
- Matching the phase: Early symptom relief is different from late-stage power development.
- Giving athletes home options: A simple recovery setup can help between visits. For athletes building a home routine, this guide to essential tools for home gym recovery is a practical place to start.
What usually doesn't work:
- Passive-only care: Getting treatment done to you without progressive loading.
- Random exercise selection: Picking drills that look hard instead of fixing the actual deficit.
- Treating pain without changing mechanics: If the pattern stays the same, symptoms usually return.
- Stopping at “feels better”: That's often too early for runners and field athletes.
For runners especially, exercise choice needs to line up with gait mechanics, loading tolerance, and training volume. This breakdown of physical therapy exercises for runners shows how those pieces connect.
The best modality is the one that helps you train better, move better, and recover well enough to keep progressing.
Sport-Specific and Population-Specific Programs
A rehab plan that works for a runner can fail a dancer. A youth soccer player doesn't need the same language, loading pattern, or coaching style as an adult post-op athlete. Sports medicine and rehab only works when it respects the demands of the person in front of you.

Runners and dancers need different plans
A runner with recurring shin, knee, or hip pain often needs more than rest and generic glute work. Running gait analysis can show whether the issue is tied to stride mechanics, cadence changes, trunk control, or poor force absorption. Then the rehab plan can match the finding. Sometimes the fix is strength. Sometimes it's training volume. Sometimes it's how the foot contacts the ground.
A dancer is different. Dance therapy needs to account for turnout, foot intrinsic control, repeated jumping, landing symmetry, hip mobility, and the fact that technique and artistic demands affect load. The plan has to support performance without flattening the movement vocabulary that makes dance possible.
Youth athletes bring another layer. They often need movement education as much as tissue recovery. If a middle school or high school athlete doesn't know how to decelerate, land, or control knee position, rehab should teach those skills early and reinforce them often.
Useful programming options for these groups include:
- Runners: Gait analysis, calf and hip strength progressions, return-to-run intervals.
- Dancers: Foot and ankle control, balance under fatigue, jump and landing mechanics.
- Youth athletes: Sprint mechanics, cutting drills, bodyweight strength, and age-appropriate power work.
If you're building a broader performance plan around rehab, a structured strength and conditioning program for athletes can help bridge the gap between rehab discharge and full sports performance.
ACL rehab needs stricter standards
ACL reconstruction is where generic rehab advice gets athletes in trouble. The athlete may feel better long before they're ready for unrestricted sport. That's why criterion-based progression matters.
Evidence shows that returning to sport after ACL reconstruction without passing specific strength and functional criteria, such as a limb symmetry index of 90% or more, increases re-injury risk fourfold according to Helix Sports Medicine's review of criterion-based ACL return to sport. That's the clinical reason not to treat “9 months” as automatic clearance.
In practice, that means ACL rehab should include:
- Strength benchmarks: The surgical leg can't stay meaningfully behind the other side.
- Hop and landing tests: Not just distance, but quality of takeoff and landing.
- Deceleration control: Clean stops, cuts, and direction changes before chaotic practice.
- Sport-specific exposure: Soccer, basketball, lacrosse, and dance all stress the knee differently.
For athletes who want extra exercise ideas between sessions, a well-organized GrabGains training library can be a useful reference, as long as the exercise selection still matches the rehab phase and your therapist's criteria.
A strong ACL rehab plan protects the athlete from doing advanced things too early, not from working hard.
Return-to-Sport Testing and Measuring Success
The end of rehab shouldn't rely on guesswork. “It feels pretty good” is encouraging, but it isn't enough for an athlete who needs to sprint, cut, jump, or absorb contact.
Why we test instead of guessing
Return-to-sport testing gives objective information about strength, power, asymmetry, control, and readiness under more realistic demands. Depending on the athlete, that can include hop testing, jump testing, single-leg control, agility drills, and strength measures that compare sides.
The key idea is simple. The body has to prove it can do the job. In post-op cases, especially ACL rehab, that often includes limb symmetry index benchmarks above 90% before full return is considered appropriate, as noted earlier in this article.
Testing also helps separate two athletes who look similar on the table but perform very differently once speed and impact are added. One athlete may have full range of motion and no swelling, yet still show a clear drop-off in landing quality or push-off power.
Confidence has to be trained too
Physical readiness is only part of the picture. After ACL surgery, 81% to 92% of athletes return to some form of activity, but only 55% to 79% return to their pre-injury level, often because confidence and psychological readiness lag behind physical clearance, according to JOSPT Open research on return-to-sport decision-making after ACL reconstruction.
That's why the final stage of sports medicine and rehab should include graded exposure to the exact situations that create hesitation. Cutting at speed. Landing in traffic. Opening up stride. Returning to overhead hitting. The athlete needs successful reps in those moments.
A useful comparison comes from other recovery paths where physical healing and real-world readiness don't always line up on the same day. For postpartum athletes returning to movement, this recovery guide for new moms is a good example of how progression needs to respect both healing and function.
Data protects athletes from returning too soon. Graded exposure helps them believe they're ready when the data says they are.
Frequently Asked Questions About Sports Rehab
Athletes and parents usually want practical answers. That's fair. Rehab works better when expectations are clear from the start.
Common questions
| Question | Answer |
|---|---|
| Do I need sports rehab if I can still practice? | Often, yes. If you're changing mechanics, losing power, or getting pain after activity, you may be compensating in ways that raise your risk of a bigger setback. |
| Will rehab just mean rest and stretching? | No. Good rehab is active. It may include temporary activity changes, but it should also rebuild strength, control, and sport-specific capacity. |
| How often will I come in? | That depends on the injury, irritability, training demands, and whether you're post-op. Some athletes need closer guidance early, then more independent training later. |
| Can younger athletes do return-to-sport testing too? | Yes. Testing should be age-appropriate, but youth and high school athletes benefit from objective measures just as much as adults do. |
| What if I'm nervous to go back even after I'm cleared? | That's common. Confidence often returns through progressive exposure, repeated successful reps, and a plan that matches your sport rather than skipping straight to full competition. |
A few final practical points
Bring your questions, your training schedule, and any imaging or surgical notes you have. Wear clothes you can move in. Expect to do more than talk.
Above all, do not wait for a minor issue to become a season-ending injury. Early sports rehab is often easier than attempting to reverse months of compensation later.
If you're dealing with pain, coming back from surgery, or trying to return to sport with more confidence, Physical Therapy U offers athlete-centered care in Bridgewater, Buzzards Bay, and Middleborough. Book an evaluation to get a plan built around your sport, your goals, and the criteria that matter.
{kind=link}