Runner’s knee is pain around or behind the kneecap, usually called patellofemoral pain syndrome (PFPS), and it affects about 25% of recreational runners each year. It’s common, frustrating, and usually very treatable, with about 70% to 90% of patients improving with targeted physical therapy interventions.
If you’re here, there’s a good chance your knee started talking back on a normal run, during stairs, after a hard practice, or halfway through a dance class. For athletes in Bridgewater, Massachusetts, across the South Shore Massachusetts area, and in towns like Plymouth, Taunton, Raynham, East Bridgewater, West Bridgewater, Buzzards Bay, and Middleborough, this is one of the most common patterns we see in sports physical therapy.
What matters most is this. Runner’s knee usually isn’t just a “bad knee.” It’s a movement problem. The kneecap isn’t tracking as cleanly as it should in its groove, and the way you load your leg, foot, hip, and trunk during training often has a lot to do with it.
Table of Contents
- That Nagging Ache What Is Runner's Knee?
- The Biomechanical Causes of Runner's Knee
- Symptoms and How a Sports PT Diagnoses PFPS
- Your Roadmap to Recovery Evidence-Based Treatments
- Long-Term Prevention for Runners and All Athletes
- Get Back in the Game with Physical Therapy U
- Frequently Asked Questions About Runner's Knee
That Nagging Ache What Is Runner's Knee?
A lot of athletes notice runner’s knee the same way. The first mile feels fine, then the front of the knee starts to ache. Or stairs suddenly feel sharper than they should after practice. Or you sit through class, work, or a long drive and your knee feels stiff and annoyed when you stand up.
What is runner’s knee? It’s the common name for patellofemoral pain syndrome, which means pain coming from the joint between the kneecap and the thigh bone. The pain is usually felt around or behind the kneecap, especially with activities that load the knee such as running, stair climbing, or deep knee bending. Research summarized at SimpleDecider’s overview of runner’s knee risk notes that PFPS affects approximately 25% of recreational runners annually and that 70% to 90% of patients improve with targeted physical therapy interventions.
That’s the part athletes need to hear early. This is common, but it shouldn’t be brushed off. If you only rest until symptoms quiet down, then jump right back into the same training with the same mechanics, the pain often returns.
Practical rule: Runner’s knee is rarely just about the knee. The real fix usually involves how you move, how you train, and how well your hips, trunk, and foot control load.
In sports physical therapy, the goal isn’t just to label the pain. It’s to answer the questions athletes care about. Why did this start? What can I keep doing? What needs to change? And what has to be true before I’m back to running, cutting, dancing, or lifting without second-guessing every step?
The Biomechanical Causes of Runner's Knee
Runner’s knee gets called an overuse injury all the time. That’s only partly true. Volume matters, but the bigger issue is often how the load moves through the leg.
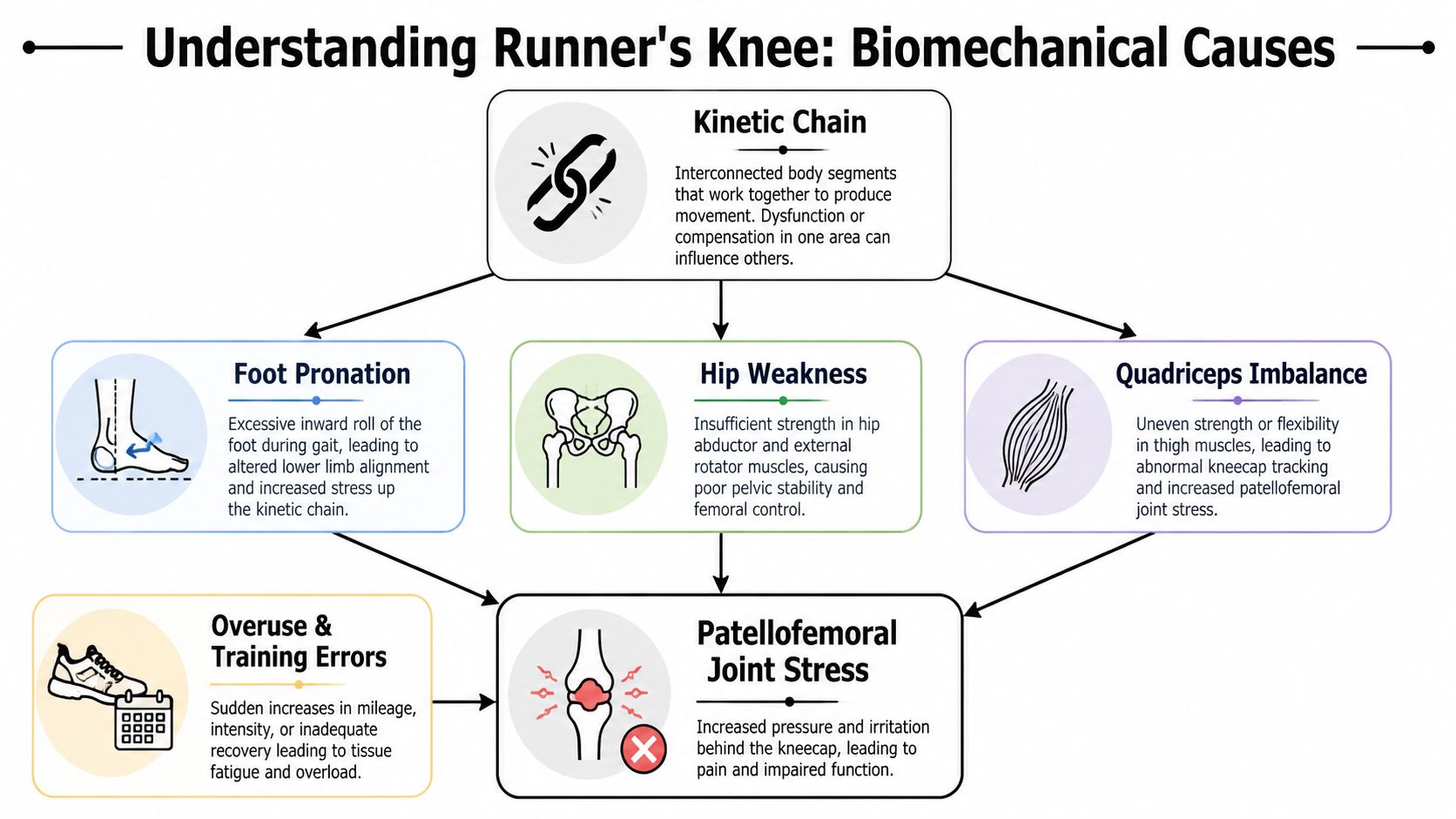
Why the kneecap gets irritated
The kneecap should glide in a groove as the knee bends and straightens. When the leg collapses inward, the femur rotates poorly, or the foot contributes to a chain of bad positions, the patella doesn’t track as cleanly. The result is more irritation at the patellofemoral joint.
This is why “just rest it” often fails as a long-term solution. Pain may calm down, but the movement pattern that created it is still there.
A useful way to think about it is the kinetic chain. Your foot, ankle, shin, knee, hip, and trunk don’t work separately during running or sport. If one segment loses control, the knee usually pays for it.
The hip driven pattern
One of the clearest patterns in PFPS is weak hip control. According to South Perth Physio’s review of the biomechanics of runner’s knee, affected subjects showed 26% reduced hip abduction strength and 36% less hip external rotation strength versus controls. The same review notes that patellofemoral joint reaction forces can reach 3 to 7 times body weight during running.
That matters clinically. If the gluteus medius and other lateral hip stabilizers can’t control the femur, the thigh rotates inward and the knee drifts into a valgus position. Athletes often describe this as feeling “wobbly,” “collapsed,” or “off” on stairs, single-leg work, or downhill running.
You can see it during a single-leg squat, landing drill, or treadmill run. The pelvis may drop. The knee caves inward. The trunk shifts to compensate. The patella gets loaded in a way it doesn’t tolerate well.
When the hip stops controlling the femur, the knee becomes the hinge that absorbs the mistake.
The foot driven pattern
The other common pathway starts lower. Excessive pronation can change how the tibia rotates, which then affects the knee above it. That doesn’t mean every flat foot causes pain, and it doesn’t mean everyone needs an insert. It means foot mechanics are part of the conversation.
The chain can also include calf stiffness. If ankle motion is restricted, the body often finds that motion elsewhere, and the knee may take more stress during running, cutting, or squatting. For athletes trying to connect tight lower legs with front-of-knee symptoms, this breakdown of calf muscles and knee discomfort is a helpful companion read.
In practice, this is why a sports PT looks beyond the painful spot. A good evaluation checks hip strength, trunk control, foot mechanics, ankle mobility, and the training decisions that exposed the problem. If your form changes as you fatigue, a running gait analysis at PTU can make those details easier to see and easier to address.
Symptoms and How a Sports PT Diagnoses PFPS
Athletes usually don’t need a lecture to know something’s wrong. They need help deciding whether the pain pattern fits runner’s knee or whether it points to something else.

What athletes usually feel
PFPS often shows up as an ache at the front of the knee or behind the kneecap. It tends to flare with loaded bending patterns and repeated impact.
Common symptom patterns include:
- Running pain: Symptoms often build during runs, especially with hills, speed changes, or longer efforts.
- Stairs and squats: Going down stairs, lunging, or deep squatting often brings it out quickly.
- Sitting stiffness: After sitting with the knee bent, the joint may feel tight or achy when you stand.
- Training disruption: Many athletes can still move, but they stop trusting the knee.
Those details matter because PFPS is often a pattern diagnosis. The story, the movement exam, and the symptom behavior all help narrow it down.
What makes a clinician look deeper
Runner’s knee is often described as a diagnosis of exclusion, which means a sports PT has to rule out other problems first. In the review summarized by this discussion of PFPS misdiagnosis and clinical testing, PFPS typically lacks true locking or instability compared with a meniscal tear or ACL injury, and up to 40% of suspected cases are misdiagnosed without proper clinical tests.
That’s why a solid sports PT exam doesn’t stop at “your kneecap hurts.” It should include:
- Movement testing: Single-leg squat, step-down, landing mechanics, and if relevant, running analysis.
- Strength testing: Especially the hips, quads, and supporting trunk control.
- Mobility screening: Ankle motion, calf flexibility, hip mobility, and tissue restrictions that alter mechanics.
- Knee-specific exam: Irritability, patellar mobility, symptom provocation, and signs that suggest something more than PFPS.
If your knee truly locks, gives way, swells aggressively, or the pain followed a clear traumatic event, don’t assume it’s runner’s knee. Get assessed in person.
A good diagnosis gives you more than a name. It gives you a plan and tells you what not to miss.
Your Roadmap to Recovery Evidence-Based Treatments
Recovery works best when athletes stop treating pain and start treating the system that created it. That means calming symptoms, restoring strength, fixing the movement fault, and then rebuilding sport tolerance in the right order.

Phase one calm it down without shutting everything down
The first mistake many athletes make is either pushing through hard pain or stopping everything. Neither extreme is ideal. The knee usually responds better to relative rest than total shutdown.
Early treatment often includes:
- Activity modification: Reduce the aggravating volume or intensity for a short window. That may mean less mileage, fewer hills, fewer deep knee loading drills, or temporary changes in practice.
- Pain-guided loading: Keep moving in ways the knee tolerates. That might include adjusted strength work, lower-impact conditioning, or shorter efforts.
- Tissue work where it helps: Soft tissue treatment can reduce guarding in the quads, lateral thigh, calves, or hip rotators when those areas are driving poor mechanics.
- Symptom support: Some athletes benefit from taping, cueing, footwear review, or temporary orthotic trials when clinically appropriate.
This is also the phase where adjunct treatments can help the athlete tolerate rehab better. For irritated soft tissue and local sensitivity, some cases respond well to sports rehab laser therapy when it’s used as part of a larger plan rather than a standalone fix.
What doesn’t work well is waiting for the knee to magically “settle down” while doing nothing to improve strength or control. Pain relief without reload usually leads to a repeat episode.
Phase two rebuild strength and control
Once symptoms are calmer, the work shifts. Now you need capacity.
The best exercise plan isn’t flashy. It’s consistent, specific, and progressed based on movement quality. Examples of useful foundations include:
- Clamshells and side-lying hip work: Good for athletes who can’t control pelvic position or femur rotation yet.
- Glute bridges and bridge progressions: Helpful when hip extension control is poor and single-leg tasks are sloppy.
- Quad sets and controlled knee extension work: Useful when the quad has shut down or the athlete avoids loading the front of the knee.
- Step-downs: Excellent for exposing valgus collapse, poor trunk control, and loss of eccentric control.
- Single-leg squats: A strong checkpoint exercise. They show whether the athlete owns the position or just survives it.
- Calf raises and ankle mobility drills: Often underrated. The foot and ankle need enough strength and motion to keep the knee from compensating.
A few practical notes matter more than the exercise menu itself:
- Tempo matters: Slow lowering phases often teach control better than rushed reps.
- Range matters: Start in a range the knee tolerates, then earn deeper loading.
- Cueing matters: “Keep the knee over the middle of the foot” is more useful than vague advice to “use better form.”
Better rehab is usually boring in the best way. You repeat high-value movements, clean up the weak links, and progress before the knee gets angry again.
Athletes also ask about shoes. That’s reasonable. Footwear won’t fix a strength or control problem by itself, but shoe choice can change how the knee feels during recovery. If you’re weighing options, this guide on carbon plate shoes for knee comfort is worth reviewing as part of a broader discussion about mechanics, training load, and tolerance.
For some athletes, dry needling fits well here too. It can reduce muscle guarding in overworked quads, calves, or hip musculature so the athlete can move more normally during strengthening. It’s not the whole plan, but it can be a useful tool inside one.
A visual demo can help if you’re trying to understand the rehab mindset before starting:
Phase three return to running jumping and sport
At this stage, athletes tend to get impatient. Pain has improved, so they assume they’re ready. Sometimes they are. Often they aren’t.
A real return-to-sport progression asks whether you can handle the demands of your sport without the old movement error reappearing when you’re tired, under speed, or on one leg. For a runner, that may mean structured return-to-run progressions and gait retraining. For a soccer or lacrosse athlete, it means controlling deceleration, cutting, and repeated efforts. For dancers, it means owning turnout, single-leg loading, and rehearsal volume.
Useful return criteria often include:
- Symptom response: The knee tolerates loading during and after activity.
- Movement quality: No obvious collapse on step-downs, hopping, or single-leg squat patterns.
- Strength confidence: You can load the leg without protecting it.
- Sport specificity: You’ve reintroduced the actual demands of your activity, not just gym exercises.
The trade-off here is simple. Returning too early protects your schedule for a week and threatens your season for a month. Taking the extra time to restore mechanics is usually the smarter athletic decision.
Long-Term Prevention for Runners and All Athletes
The best prevention plan is not a random list of exercises. It’s a habit system that keeps the knee from drifting back into the same overload pattern.

What actually lowers recurrence risk
Most prevention advice fails because it’s too generic. “Stretch more” and “listen to your body” aren’t enough for competitive athletes.
What works better is a repeatable routine:
- Keep hip strength in your week: If your glutes stop doing their job, the knee usually notices first.
- Warm up with intent: Use drills that prepare landing, deceleration, and single-leg control rather than a few rushed static stretches.
- Watch training spikes: Sudden jumps in mileage, hills, plyometrics, or practice intensity are common triggers.
- Build tissue tolerance year-round: Off-season strength work is what makes in-season load possible.
- Use feedback tools: Video, coaching cues, and app-based programming help athletes stay more consistent than memory alone.
For athletes who want structure outside the clinic, a guided home program through the PTU running app can help keep mobility, strength, and progression from becoming guesswork.
Why dancers and court sport athletes need the same conversation
Runner’s knee isn’t only a runner problem. Dancers, field sport athletes, and youth players with high practice volume deal with the same patellofemoral stress pattern, just through different movements.
That’s one reason old alignment myths don’t hold up well. According to WebMD’s overview of runner’s knee and PFPS, a larger Q-angle is not a predictor of pain, and hip abductor weakness drives up to 70% of cases in female athletes. That shifts the focus away from blaming static anatomy and toward improving strength and control.
Prevention gets more effective when you stop chasing perfect alignment and start building repeatable control under fatigue.
For dancers, that may mean hip and trunk strength that supports turnout and repeated plié work. For youth athletes, it often means better landing mechanics and enough recovery between practices, games, lifting, and skill sessions. For post-op athletes returning from ACL rehab, it means not assuming the knee is ready just because the calendar says it should be.
Get Back in the Game with Physical Therapy U
Athletes around Bridgewater, Massachusetts, Buzzards Bay, and Middleborough don’t need generic rehab for a sports problem. They need sports physical therapy that looks at movement, load, and performance together.
At Physical Therapy U, care is built for athletes from youth and high school competitors to adult runners, dancers, and post-surgical patients working back from ACL reconstruction and other orthopedic setbacks. That means one-on-one treatment with licensed DPTs, not a handout and a few bands.
What stands out is the full return-to-sport lens. That includes running gait analysis, dry needling, myofascial release, dance therapy, recovery tools such as NormaTec, and performance-based return testing that helps answer the question athletes actually ask: “Am I ready?”
That approach matters whether you live in Bridgewater, Plymouth, Taunton, Raynham, East Bridgewater, West Bridgewater, Buzzards Bay, or Middleborough. If your front-of-knee pain is limiting running, lifting, practice, or confidence, stop guessing and get a proper sports PT evaluation.
Frequently Asked Questions About Runner's Knee
| Question | Answer |
|---|---|
| Can I keep running with runner’s knee? | Sometimes, yes, but only if symptoms stay manageable and your knee isn’t getting worse during or after runs. Many athletes do better with temporary mileage, hill, or pace changes instead of pushing through the same load. |
| Do knee braces fix PFPS? | A brace may help some athletes feel more supported, but it usually doesn’t solve the reason the pain started. Long-term improvement usually comes from strength, movement retraining, and smart load progression. |
| Is rest enough? | Rest can calm symptoms, but it usually doesn’t correct the hip, foot, or training issues behind the pain. That’s why symptoms often return when training resumes. |
| Does everyone with kneecap pain have runner’s knee? | No. Front-of-knee pain can come from several different problems. If you have locking, instability, major swelling, or pain after a traumatic event, get examined in person. |
| How long does recovery take? | Recovery depends on irritability, training demands, and how consistent you are with rehab. The most useful timeline is based on restored function, not just waiting a set number of days. |
If runner’s knee is changing how you run, train, dance, or recover, book an evaluation with Physical Therapy U. Our sports PT team in Bridgewater, Buzzards Bay, and Middleborough helps athletes across Southeastern Massachusetts identify the underlying cause of knee pain, build a clear rehab plan, and return to sport with confidence.
{kind=link}